


OBI=on-body injector.
ACCESS
FOR SKYRIZI
SKYRIZI Has >95% Coverage in Crohn’s and UC
MEDICAL BENEFIT

COMMERCIAL
coverage2*
coverage2*
PHARMACY BENEFIT
PREFERRED
first-line commercial TIM coverage2*†
first-line commercial TIM coverage2*†
National Commercial Formulary Coverage as of August 20252*
Any eligible, commercially insured patient who experiences a 5-day delay‡ in approval or is denied will be approved for a no-charge shipment of SKYRIZI.‡
PREFERRED FIRST-LINE TIM COVERAGE MEANS SKYRIZI IS AVAILABLE:
- For CD: No step through of biologic
- For UC: No step through of biologics and S1P receptor modulators
- At the lowest branded copay/coinsurance tier
Get Your Patients Started
*Coverage requirements and benefit designs vary by payer and may change over time. Please consult with payers directly for the most current reimbursement policies. Medical coverage may require a step edit depending on the plan’s management.
†SKYRIZI is on a preferred tier or otherwise has preferred status on the plan’s formulary.
‡For patients pending insurance approval of their medical benefit for the SKYRIZI IV induction dose.
IV=intravenous; S1P=Sphingosine-1-phosphate; TIM=targeted immunomodulator.
Three Reasons to Enroll Your Patients in Skyrizi Complete
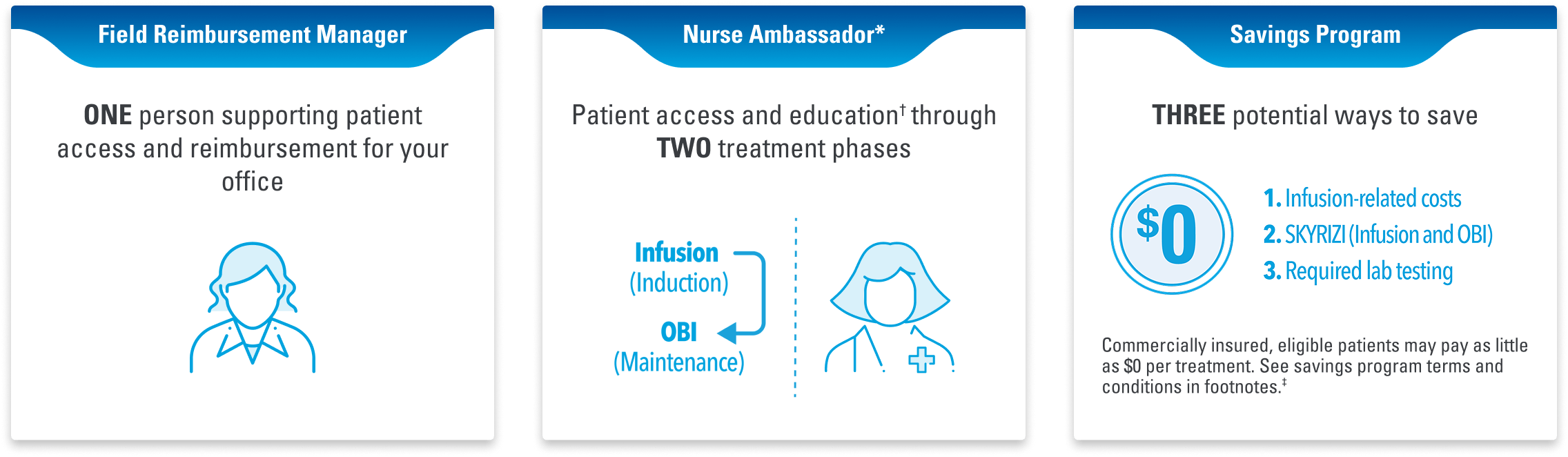
When your office or infusion center enrolls patients, Skyrizi Complete also provides access to these services:
- Patient Savings Card information
- Proactive Field Reimbursement Manager Support
- Proactive Plan Benefits Verification conducted
- Proactive bridge support for delays in Prior Authorization approvals
- Nurse Ambassador
*Nurse Ambassadors are provided by AbbVie and do not provide medical advice or work under the direction of the prescribing health care professional (HCP). They are trained to direct patients to speak with their HCP about any treatment-related questions, including further referrals.
†Patient access and education includes processes and information around patient coverage through the benefits verification (BV) and prior authorization (PA) process for both the infusion and on-body injector (OBI).
‡Eligibility: Available to patients with commercial insurance coverage for SKYRIZI® (risankizumab-rzaa) who meet eligibility criteria. This co-pay assistance program is not available to patients receiving prescription reimbursement under any federal, state, or government-funded insurance programs (for example, Medicare [including Part D], Medicare Advantage, Medigap, Medicaid, TRICARE, Department of Defense, or Veterans Affairs programs) or where prohibited by law. Offer subject to change or termination without notice. Restrictions, including monthly maximums, may apply. This is not health insurance. For full Terms and Conditions, visit www.SKYRIZICDSavingsCard.com or call 1.866.SKYRIZI for additional information. To learn about AbbVie’s privacy practices and your privacy choices, visit https://abbv.ie/corpprivacy.
Choose the Right Enrollment Form for Your Office
HCP Office Enrollment
Infusion Site Enrollment
HCP=healthcare provider.
Recommended for You
Skyrizi Complete
Dosing