


OBI=on-body injector.
ACCESS
FOR SKYRIZI
SKYRIZI has >95% Preferred National Commercial and Medicare Part D Coverage in UC and CD2*†
MEDICAL BENEFIT

COMMERCIAL
coverage2*
coverage2*
PHARMACY BENEFIT
PREFERRED
first-line TIM commercial and Medicare Part D coverage2*†
first-line TIM commercial and Medicare Part D coverage2*†
National Commercial Formulary Coverage as of May 20262
Any eligible, commercially insured patient who experiences a 5-day delay‡ in approval or is denied will be approved for a no-charge shipment of SKYRIZI.‡§
PREFERRED FIRST-LINE TIM COVERAGE CAN MEAN SKYRIZI IS AVAILABLE:
- For CD: No step through of biologic
- For UC: No step through of biologics and S1P receptor modulators
Get Your Patients Started
*Coverage requirements and benefit designs vary by payer and may change over time. Please consult with payers directly for the most current reimbursement policies.
†SKYRIZI is on a preferred tier or otherwise has preferred status on the plan’s formulary.
‡For patients pending insurance approval of their medical benefit for the SKYRIZI IV induction dose.
§Eligibility criteria: Available to patients aged 63 or younger with commercial insurance coverage. Patients must have a valid prescription for SKYRIZI® (risankizumab-rzaa) for an FDA-approved indication and a denial of insurance coverage based on a prior authorization request on file along with a confirmation of appeal. For medical coverage, a delay of more than 5 business days or denial of treatment coverage from their insurance will be required. Continued eligibility for the program requires the submission of an appeal of the coverage denial every 180 days. Program provides for SKYRIZI® (risankizumab-rzaa) at no charge to patients for up to two years or until they receive insurance coverage approval, whichever occurs earlier, and is not contingent on purchase requirements of any kind. Program is not available to patients whose medications are reimbursed in whole or in part by Medicare, Medicaid, TRICARE, or any other federal or state program. Offer subject to change or discontinuance without notice. This is not health insurance and program does not guarantee insurance coverage. No claims for payment may be submitted to any third party for product dispensed by program. Limitations may apply.
IV=intravenous; S1P=Sphingosine-1-phosphate; TIM=targeted immunomodulator.
Check the Formulary Status for SKYRIZI in Your Area
Select a filter
Choose Indication
This site is protected by reCAPTCHA and the Google
Privacy Policy and
Terms of Service apply.
Top Medical Plans Covering SKYRIZI IV**††
- Insurance plan
- Status
**Coverage requirements and benefits designs vary by payer and may change over time. Please consult with payers directly for the most current reimbursement policies. The health plans and/or pharmacy benefit managers listed here have not endorsed and are not affiliated with this material.
††Formulary Definitions:
- Covered without Biologic Step means that the medical policy covers patients to labeled indication, with no additional biologic steps that the patient needs to fail to before starting therapy.
- Covered with 1 Biologic Step means that the medical policy requires a patient to first try and fail one biologic before being approved to start therapy.
- Covered with 2 or more Biologic Steps means that the medical policy requires a patient to first try and fail two or more biologics before being approved to start therapy.
- Non-preferred means SKYRIZI may require a step edit or a higher out-of-pocket cost, be placed on a higher formulary tier, and/or require the meeting of other restrictive criteria.
‡‡For Crohn’s, advanced therapy is defined as biologics. For UC, advanced therapy is defined as biologics and S1P receptor modulators.
IV=intravenous; S1P=sphingosine-1-phosphate; SC=subcutaneous; UC=ulcerative colitis.
§§Preferred means SKYRIZI is on a preferred tier or otherwise has preferred status on the plan’s formulary.
Top Pharmacy Plans Covering SKYRIZI SC as a Preferred First-Line Advanced Therapy**††‡‡§§
- Insurance plan
- Status
**Coverage requirements and benefits designs vary by payer and may change over time. Please consult with payers directly for the most current reimbursement policies. The health plans and/or pharmacy benefit managers listed here have not endorsed and are not affiliated with this material.
††Formulary Definitions:
- Covered without Biologic Step means that the medical policy covers patients to labeled indication, with no additional biologic steps that the patient needs to fail to before starting therapy.
- Covered with 1 Biologic Step means that the medical policy requires a patient to first try and fail one biologic before being approved to start therapy.
- Covered with 2 or more Biologic Steps means that the medical policy requires a patient to first try and fail two or more biologics before being approved to start therapy.
- Non-preferred means SKYRIZI may require a step edit or a higher out-of-pocket cost, be placed on a higher formulary tier, and/or require the meeting of other restrictive criteria.
‡‡For Crohn’s, advanced therapy is defined as biologics. For UC, advanced therapy is defined as biologics and S1P receptor modulators.
IV=intravenous; S1P=sphingosine-1-phosphate; SC=subcutaneous; UC=ulcerative colitis.
§§Preferred means SKYRIZI is on a preferred tier or otherwise has preferred status on the plan’s formulary.
Three Reasons to Enroll Your Patients in Skyrizi Complete
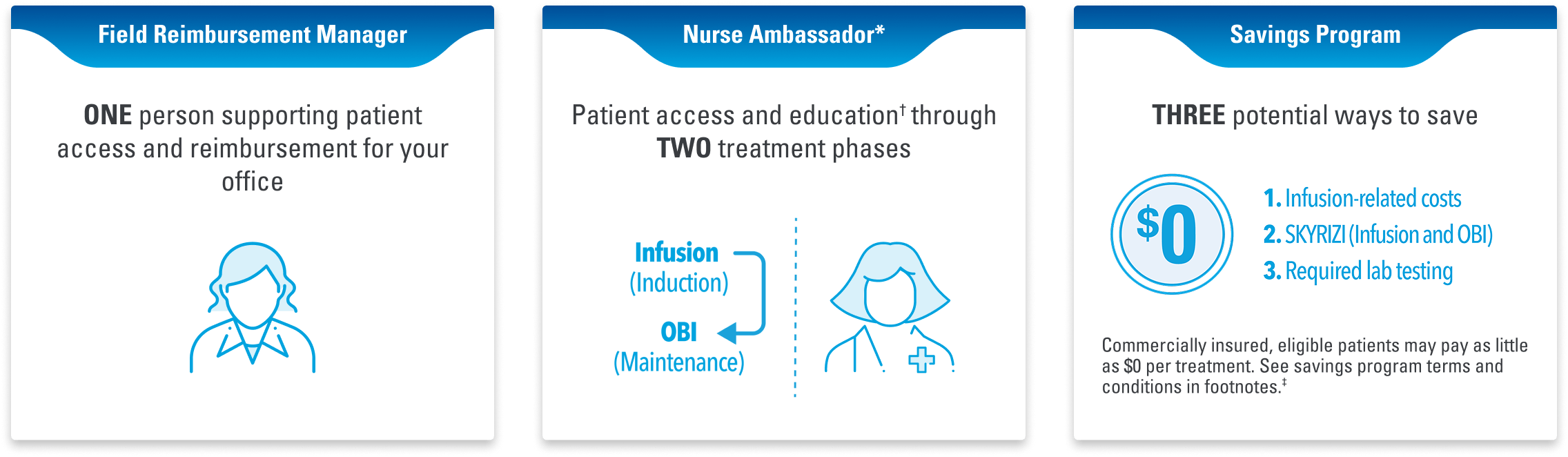
When your office or infusion center enrolls patients, Skyrizi Complete also provides access to these services:
- Patient Savings Card information
- Proactive Field Reimbursement Manager Support
- Proactive Plan Benefits Verification conducted
- Proactive bridge support for delays in Prior Authorization approvals
- Nurse Ambassador
IINurse Ambassadors are provided by AbbVie and do not provide medical advice or work under the direction of the prescribing health care professional (HCP). They are trained to direct patients to speak with their HCP about any treatment-related questions, including further referrals.
¶Patient access and education includes processes and information around patient coverage through the benefits verification (BV) and prior authorization (PA) process for both the infusion and on-body injector (OBI).
#Eligibility: Available to patients with commercial insurance coverage for SKYRIZI® (risankizumab-rzaa) who meet eligibility criteria. This co-pay assistance program is not available to patients receiving prescription reimbursement under any federal, state, or government-funded insurance programs (for example, Medicare [including Part D], Medicare Advantage, Medigap, Medicaid, TRICARE, Department of Defense, or Veterans Affairs programs) or where prohibited by law. Offer subject to change or termination without notice. Restrictions, including monthly maximums, may apply. This is not health insurance. For full Terms and Conditions, visit www.SKYRIZICDSavingsCard.com or call 1.866.SKYRIZI for additional information. To learn about AbbVie’s privacy practices and your privacy choices, visit https://abbv.ie/corpprivacy.
Choose the Right Enrollment Form for Your Office
HCP Office Enrollment
Infusion Site Enrollment
HCP=healthcare provider.
Recommended for You
Skyrizi Complete
Dosing