


For patients 6 years of age and older with moderate to severe plaque psoriasis (Ps) who are candidates for systemic therapy or phototherapy or with active psoriatic arthritis (PsA).1
Now approved for pediatric patients
US-MULT-250253
An IL-23 inhibitor from AbbVie for patients 6 years of age and older with
moderate to severe plaque psoriasis (Ps) who are candidates for systemic
therapy or phototherapy or with active psoriatic arthritis (PsA).1
Nothing less than the opportunity for skin and joint efficacy data. For your patients, that's everything.
Nothing less than the opportunity for skin and joint efficacy data.
For your patients, that's everything.

PASI 90=≥90% improvement in Psoriasis Area and Severity Index; PASI 100=100% improvement in Psoriasis Area and Severity Index; sPGA 0/1=static Physician’s Global Assessment rating of clear or almost clear.
THE ONLY 4-DOSE-A-YEAR SYSTEMIC FOR PSORIASIS AND FOR PSORIATIC ARTHRITIS THAT OFFERS A SINGLE-DOSE PEN1
*Based on combined prescription data across Ps and PsA, excluding generics and OTC.4‡
†"First-line" is defined as the first biologic among patients who have not been prescribed one in the last 3 years.5,6§
‡Source of data: Integrated Symphony Health as of 8/2025. The term branded systemic is defined as systemic drugs that are sold by a specific name or trademark and protected by patent. OTC stands for over-the-counter medications.
§Source: Integrated Symphony Health (PatientSource) and IQVIA (NSP and NPA) through proprietary method of diagnosis classification. Prescriptions from rheumatologists as of 10/2025 and dermatologists as of 10/2025.
PREFERRED‖ COMBINED NATIONAL COMMERCIAL AND MEDICARE PART D FORMULARY COVERAGE UNDER THE PHARMACY BENEFIT AS OF APRIL 2026 IN Ps AND PsA7¶
‖SKYRIZI is on a preferred tier or otherwise has preferred status on the plan’s formulary.
¶Coverage requirements and benefit designs vary by payer and may change over time. Please consult with payers directly for the most current reimbursement policies.
Indication and Important Safety Information, including BOXED WARNING for Serious Infections and Malignancy. See
#Evaluated in patients with moderate plaque psoriasis eligible for systemic therapy.
**SOURCING: In this study, 46 patients outside of the US received non–US-licensed secukinumab. Data regarding comparability between US and non-US secukinumab are not publicly available.12
††ACTIVE COMPARATOR: The ustekinumab used as a biologic active control in UltIMMa-1 and UltIMMa-2 was sourced from the European Union. Comparability between non–US-approved ustekinumab and US-approved ustekinumab has not been established.
Products and their designs are trademarks of their respective owners.
5 MOAs refers only to agents listed.
AT WEEK 161,2: 75% OF SKYRIZI PATIENTS (n=220/294) ACHIEVED PASI 90 in the UltIMMa-2 study vs 2% of placebo patients (n=2/98);
84% of SKYRIZI patients achieved sPGA 0/1 vs 5% of placebo patients
UltlMMa-1 results at Week 16
PASI 90: SKYRIZI 75% (n=304), placebo 5% (n=102)
sPGA 0/1: SKYRIZI 88% (n=304), placebo 8% (n=102)
Co-primary endpoints for UltIMMa-1 and -2 were PASI 90 and sPGA 0/1 response vs placebo at Week 16.
p<0.0001 for comparisons of SKYRIZI vs placebo
STUDY DESIGN:
UltIMMa-1 (N=506) and UltIMMa-2 (N=491) were replicate Phase 3, randomized, double-blind, placebo- and active-controlled studies to evaluate the efficacy and safety of SKYRIZI (150 mg) vs placebo over 16 weeks and biologic active control (45 mg or 90 mg, based on screening weight) over 52 weeks in adult patients with moderate to severe plaque psoriasis.1,2


AT WEEK 521,2: 81% OF SKYRIZI PATIENTS (n=237/294) ACHIEVED PASI 90 in the UltIMMa-2 study; placebo did not continue beyond Week 16
UltlMMa-1 results at Week 52
PASI 90: SKYRIZI 82% (n=249/304), placebo n/a
Co-primary endpoints for UltIMMa-1 and -2 were PASI 90 and sPGA 0/1 response vs placebo at Week 16.
p<0.0001 for comparisons of SKYRIZI vs placebo
STUDY DESIGN:
UltIMMa-1 (N=506) and UltIMMa-2 (N=491) were replicate Phase 3, randomized, double-blind, placebo- and active-controlled studies to evaluate the efficacy and safety of SKYRIZI (150 mg) vs placebo over 16 weeks and biologic active control (45 mg or 90 mg, based on screening weight) over 52 weeks in adult patients with moderate to severe plaque psoriasis.1,2
EXPLORE LONG-TERM DATA
In adults, SKYRIZI has long-term efficacy data in Ps (~6 years) and PsA (~4 years) and long-term safety data (~9 years in Ps, 5 years in PsA)13-16

Complete Pro is a flexible and easy-to-use portal designed to streamline and manage the prescription process to help patients start and stay on track with their prescribed treatment.

National commercial formulary coverage under the pharmacy benefit as of April 2026
Eligible patients may be able to access their SKYRIZI at no charge until their insurance plan covers SKYRIZI or up to 2 years, whichever occurs earlier.‖‖
‡‡SKYRIZI is on a preferred tier or otherwise has preferred status on the plan’s formulary.
§§Coverage requirements and benefit designs vary by payer and may change over time. Please consult with payers directly for the most current reimbursement policies.
‖‖Eligibility criteria: Available to patients aged 63 or younger with commercial insurance coverage. Patients must have a valid prescription for SKYRIZI® (risankizumab-rzaa) for an FDA approved indication and a denial of insurance coverage based on a prior authorization request on file along with a confirmation of appeal. Continued eligibility for the program requires the submission of an appeal of the coverage denial every 180 days. Program provides for SKYRIZI® (risankizumab-rzaa) at no charge to patients for up to two years or until they receive insurance coverage approval, whichever occurs earlier, and is not contingent on purchase requirements of any kind. Program is not available to patients whose medications are reimbursed in whole or in part by Medicare, Medicaid, TRICARE, or any other federal or state program. Offer subject to change or discontinuance without notice. This is not health insurance and program does not guarantee insurance coverage. No claims for payment may be submitted to any third party for product dispensed by program. Limitations may apply.
Plaque Psoriasis: SKYRIZI is indicated for the treatment of moderate to severe plaque psoriasis in adults and pediatric patients 6 years of age and older who are candidates for systemic therapy or phototherapy.
Psoriatic Arthritis: SKYRIZI is indicated for the treatment of active psoriatic arthritis in adults and pediatric patients 6 years of age and older.
Hypersensitivity Reactions
SKYRIZI® (risankizumab-rzaa) is contraindicated in patients with a history of serious hypersensitivity reaction to risankizumab-rzaa or any of the excipients. Serious hypersensitivity reactions, including anaphylaxis, have been reported with the use of SKYRIZI. If a serious hypersensitivity reaction occurs, discontinue SKYRIZI and initiate appropriate therapy immediately.
Infection
SKYRIZI may increase the risk of infection. Do not initiate treatment with SKYRIZI in patients with a clinically important active infection until it resolves or is adequately treated.
In patients with a chronic infection or a history of recurrent infection, consider the risks and benefits prior to prescribing SKYRIZI. Instruct patients to seek medical advice if signs or symptoms of clinically important infection occur. If a patient develops such an infection or is not responding to standard therapy, closely monitor and discontinue SKYRIZI until the infection resolves.
Tuberculosis (TB)
Prior to initiating treatment with SKYRIZI, evaluate for TB infection and consider treatment in patients with latent or active TB for whom an adequate course of treatment cannot be confirmed. Monitor patients for signs and symptoms of active TB during and after SKYRIZI treatment. Do not administer SKYRIZI to patients with active TB.
Immunizations
Avoid use of live vaccines in patients treated with SKYRIZI. Drugs that interact with the immune system may increase the risk of infection following administration of live vaccines. Prior to initiating SKYRIZI, complete all age appropriate vaccinations according to current immunization guidelines.
Adverse Reactions
Most common (≥1%) adverse reactions associated with SKYRIZI include upper respiratory infections, headache, fatigue, injection site reactions, and tinea infections.
In psoriatic arthritis phase 3 trials, the incidence of hepatic events was higher with SKYRIZI compared to placebo.
SKYRIZI is available in a 150 mg/mL prefilled syringe and pen, and a 55 mg/0.37 mL prefilled syringe.
Please see Full Prescribing Information.
US-SKZD-260364
REFERENCES
For patients 6 years of age and older with moderate to severe plaque psoriasis (Ps) who are candidates for systemic therapy or phototherapy or with active psoriatic arthritis (PsA).1
Now approved for pediatric patients
ONLY IL-23i APPROVED FOR Ps OR PsA IN PATIENTS AGES 6+ WEIGHING LESS THAN 40 kg1
SKYRIZI is only 4 doses a year after 2 initiation doses at Weeks 0 and 4 as a 55 mg/0.37 mL prefilled syringe for patients weighing less than 40 kg, or as a 150 mg/mL prefilled syringe or pen for patients weighing 40 kg or more.
REFERENCE: 1. SKYRIZI [package insert]. North Chicago, IL: AbbVie Inc.
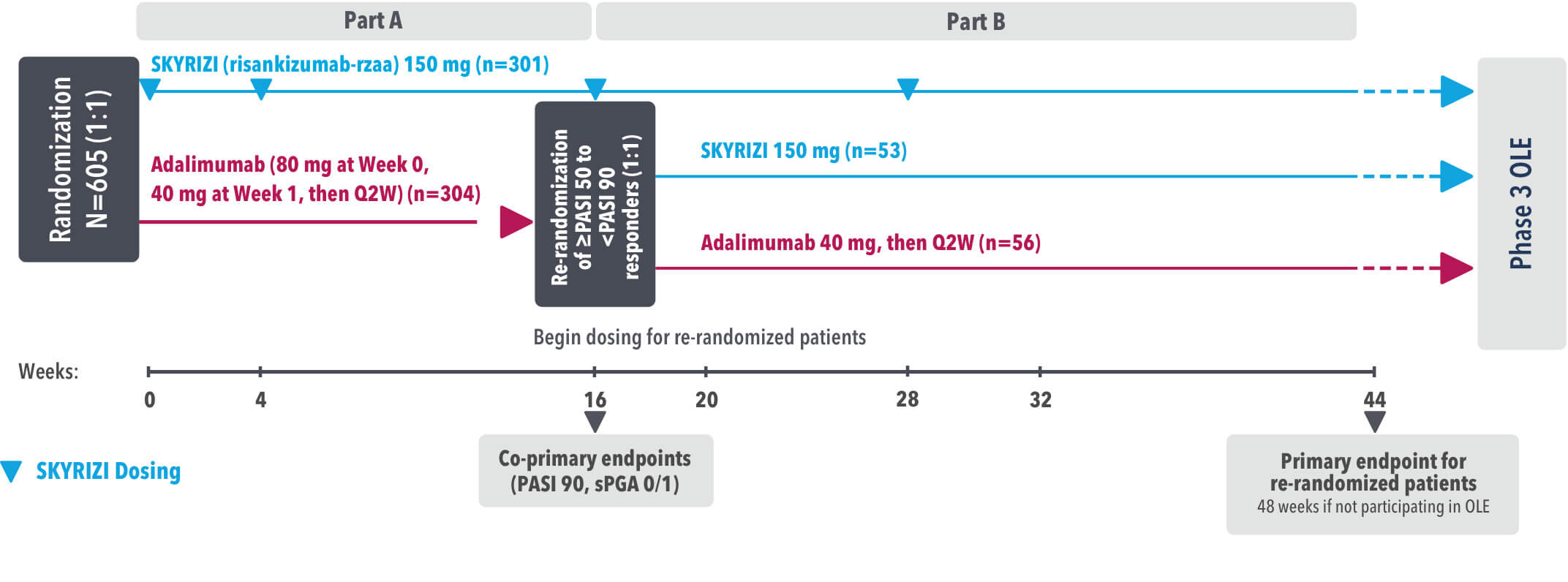
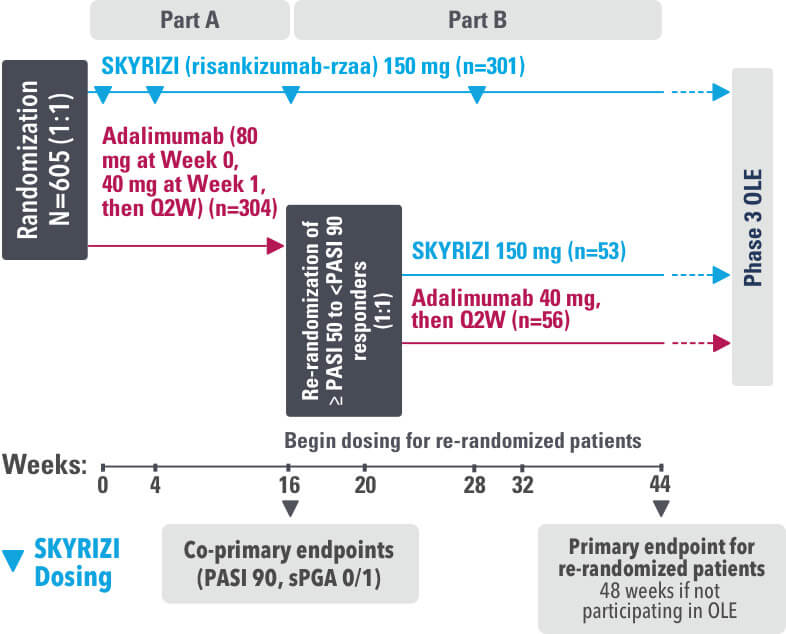
IMMvent was a Phase 3, randomized, double-blind, double-dummy, active-controlled study to evaluate the efficacy and safety of SKYRIZI (150 mg) compared to HUMIRA® (adalimumab) in adult patients with moderate to severe plaque psoriasis over 44 weeks.
Patients treated with adalimumab during Part A:
Part A
In the first phase, patients were randomized 1:1 to either SKYRIZI (150 mg), given as a subcutaneous injection at Weeks 0 and 4 and every 12 weeks thereafter or HUMIRA, given as a subcutaneous injection, with an initial dose of 80 mg followed by 40 mg every other week starting 1 week after the initial dose over 44 weeks.
The Part A co-primary endpoints were
Part B
Patients originally randomized to SKYRIZI received it throughout the study (Parts A & B). Among patients originally randomized to receive HUMIRA, those with a PASI 50 but less than PASI 90 response were re-randomized 1:1 to switch to SKYRIZI or continue HUMIRA.
The Part B primary endpoint was
Key secondary endpoints included
Key inclusion criteria
OLE=Open-Label Extension
PASI=Psoriasis Area and Severity Index
PASI 90=≥90% improvement in Psoriasis Area and Severity Index
PASI 100=100% improvement in Psoriasis Area and Severity Index
Q2W=Once every 2 weeks
sPGA=static Physician's Global Assessment
Click to see HUMIRA® (adalimumab) Indication and Important Safety Information, including BOXED WARNING for Serious Infections and Malignancy
OLE=Open-Label Extension
PASI=Psoriasis Area and Severity Index
PASI 90=≥90% improvement in Psoriasis Area and Severity Index
PASI 100=100% improvement in Psoriasis Area and Severity Index
Q2W=Once every 2 weeks
sPGA=static Physician's Global Assessment
Reference
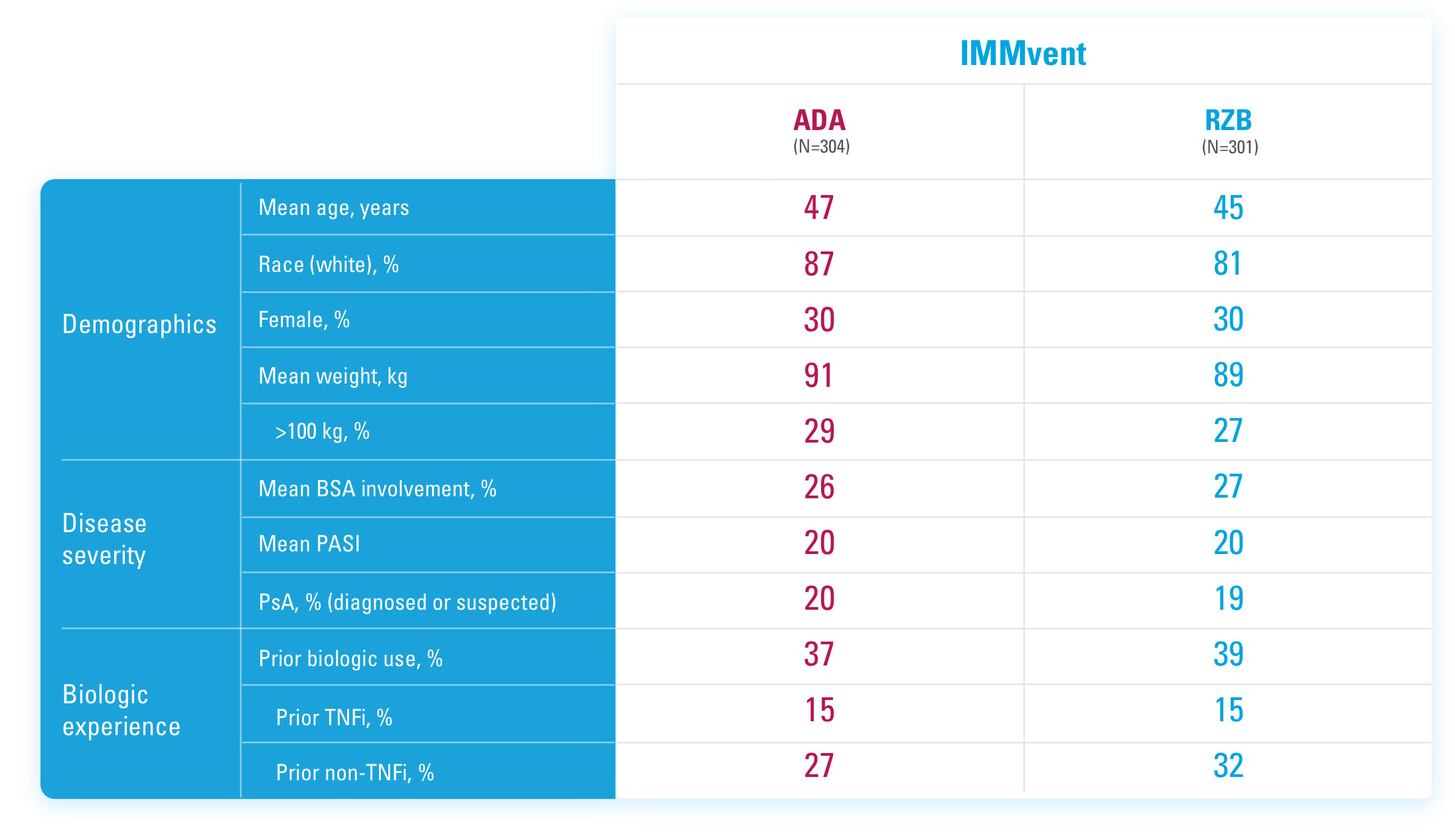
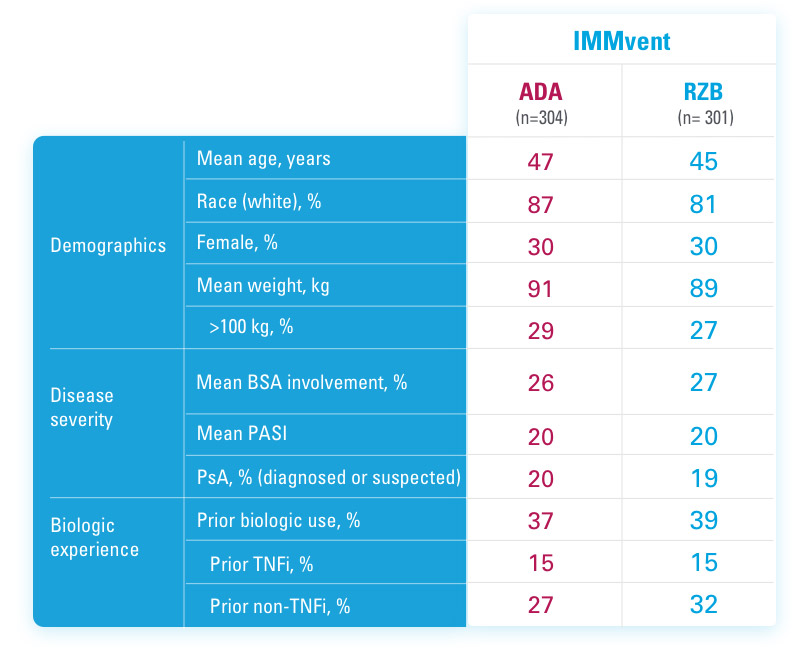
ADA=adalimumab
BSA=Body Surface Area
PASI=Psoriasis Area and Severity Index
PsA=Psoriatic Arthritis
RZB=risankizumab-rzaa
TNFi=Tumor Necrosis Factor Inhibitor
References
US-SKZD-220459
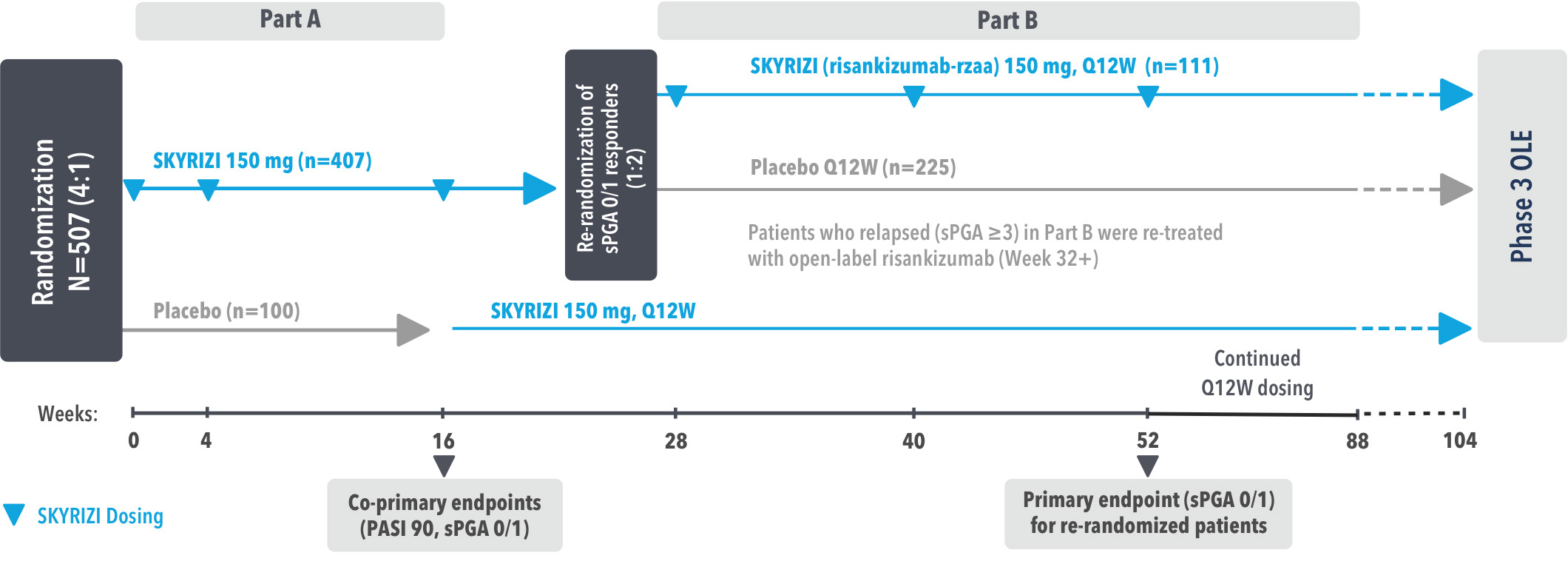
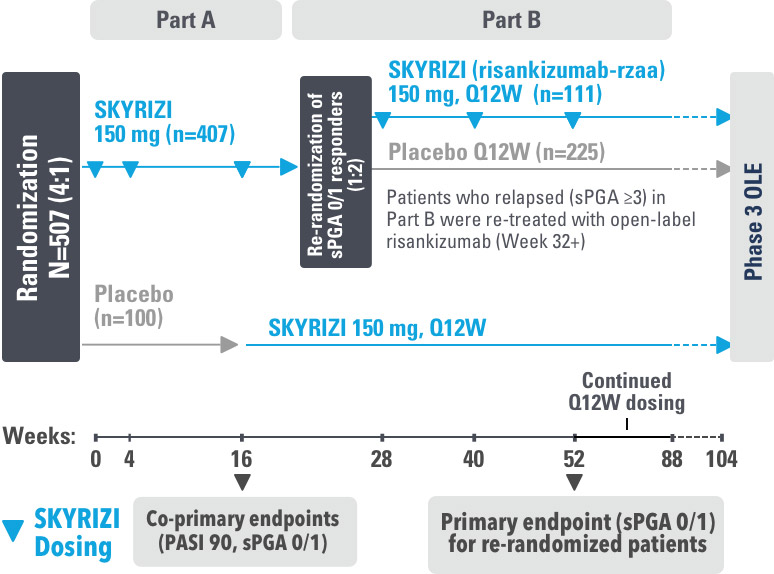
IMMhance was a Phase 3, multicenter, randomized, double-blind, placebo-controlled study to evaluate the impact of treatment withdrawal and re-treatment of SKYRIZI compared to placebo in adult patients with moderate to severe plaque psoriasis.
Part A
In the first phase, patients were randomized 4:1 to SKYRIZI (150 mg), given as a subcutaneous injection at baseline, 4 weeks later, and every 12 weeks thereafter, or placebo.
The Part A co-primary endpoints were
Part B
In the second phase of this study (Week 28 through Week 104), patients originally randomized to SKYRIZI who achieved sPGA 0/1 at Week 28 were re-randomized (1:2) to SKYRIZI (maintenance) or placebo (withdrawal). Beginning at Week 28, patients with sPGA ≥2 continued on SKYRIZI (150 mg) once every 12 weeks up to Week 88, with a final follow-up at Week 104.
The Part B primary endpoint was
Key inclusion criteria
Key secondary endpoints included
DLQI=Dermatology Life Quality Index
OLE=Open-Label Extension
PASI=Psoriasis Area and Severity Index
PASI 75=≥75% improvement in Psoriasis Area and Severity Index
PASI 90=≥90% improvement in Psoriasis Area and Severity Index
PASI 100=100% improvement in Psoriasis Area and Severity Index
Q12W=Once every 12 weeks
sPGA=static Physician's Global Assessment
References
BSA=Body Surface Area
PASI=Psoriasis Area and Severity Index
PBO=Placebo
PsA=Psoriatic Arthritis
RZB=risankizumab-rzaa
TNFi=Tumor Necrosis Factor Inhibitor
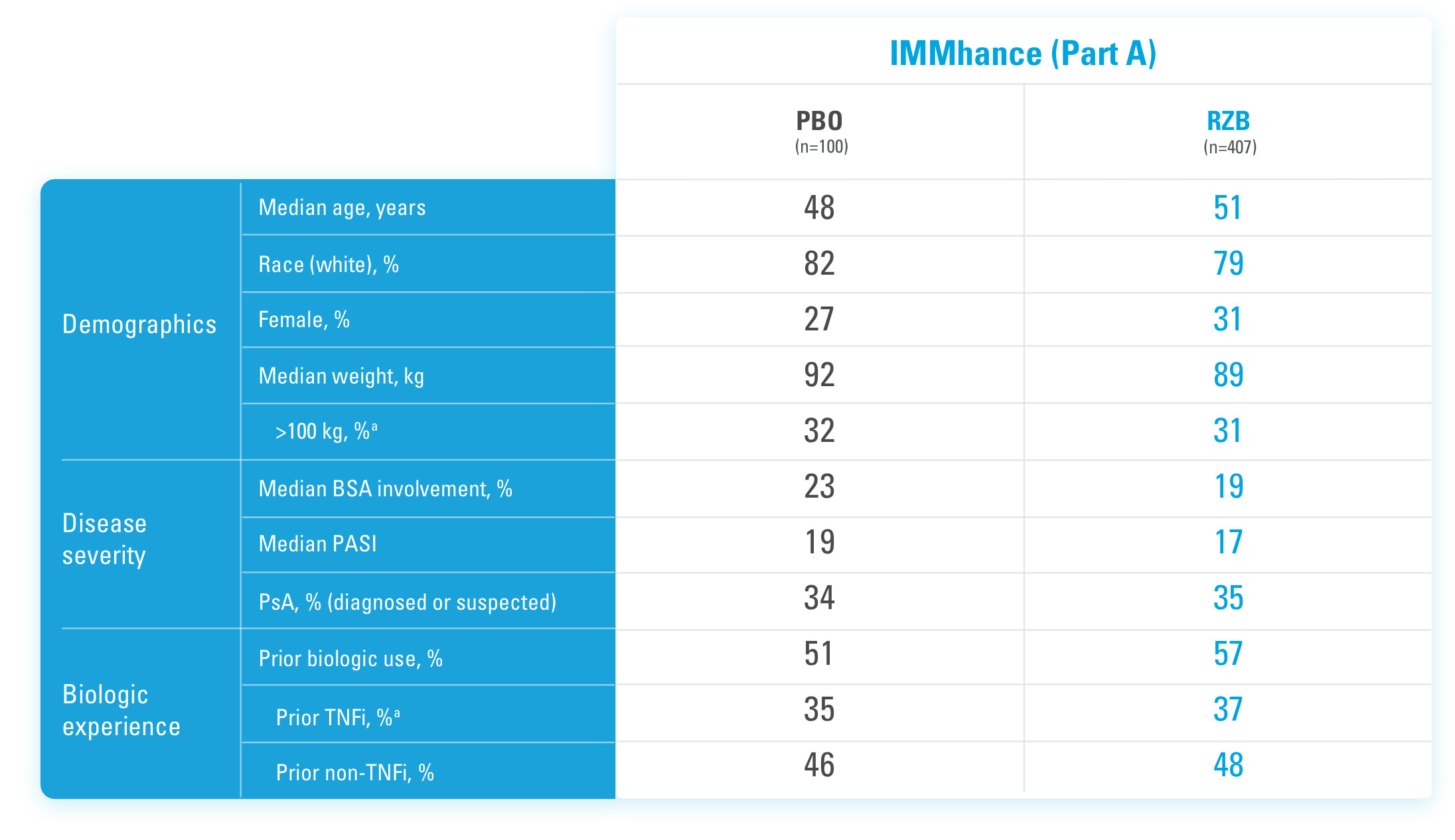
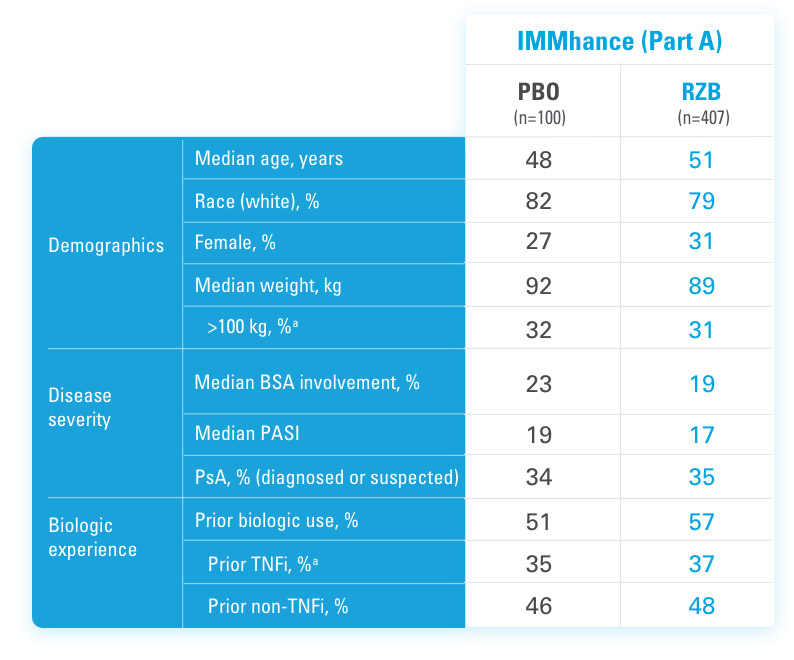
aStratification factors at randomization.
References
US-SKZD-220459
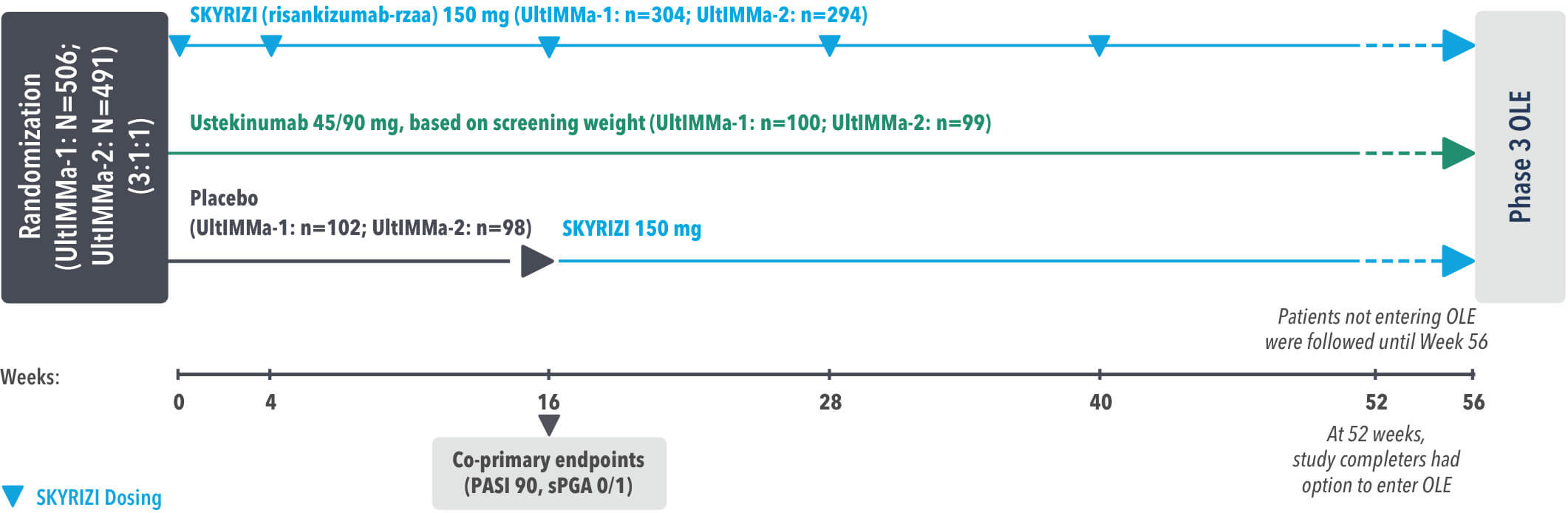
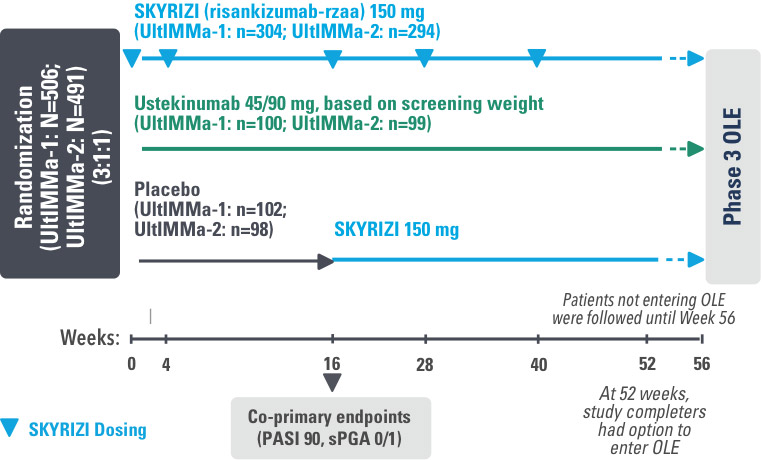
UltIMMa-1 (N=506) and UltIMMa-2 (N=491) were replicate Phase 3, randomized, double-blind, placebo- and active-controlled studies to evaluate the efficacy and safety of SKYRIZI (150 mg) vs placebo over 16 weeks and biologic active control (45 mg or 90 mg, based on screening weight) over 52 weeks in adult patients with moderate to severe plaque psoriasis. SKYRIZI (150 mg) was given as 2 subcutaneous injections at Weeks 0, 4, 16, 28, and 40. Patients were randomized 3:1:1 to receive SKYRIZI, ustekinumab, or placebo. At Week 16, patients on placebo were switched to SKYRIZI.
Active comparator
The active comparator (ustekinumab) used for these studies was sourced from the European Union.
OLE=Open-Label Extension
PASI=Psoriasis Area and Severity Index
PASI 90=≥90% improvement in Psoriasis Area and Severity Index
PASI 100=100% improvement in Psoriasis Area and Severity Index
sPGA=static Physician's Global Assessment
The co-primary endpoints were
Key secondary endpoints included
Key inclusion criteria
OLE=Open-Label Extension
PASI=Psoriasis Area and Severity Index
PASI 90=≥90% improvement in Psoriasis Area and Severity Index
PASI 100=100% improvement in Psoriasis Area and Severity Index
sPGA=static Physician's Global Assessment
References
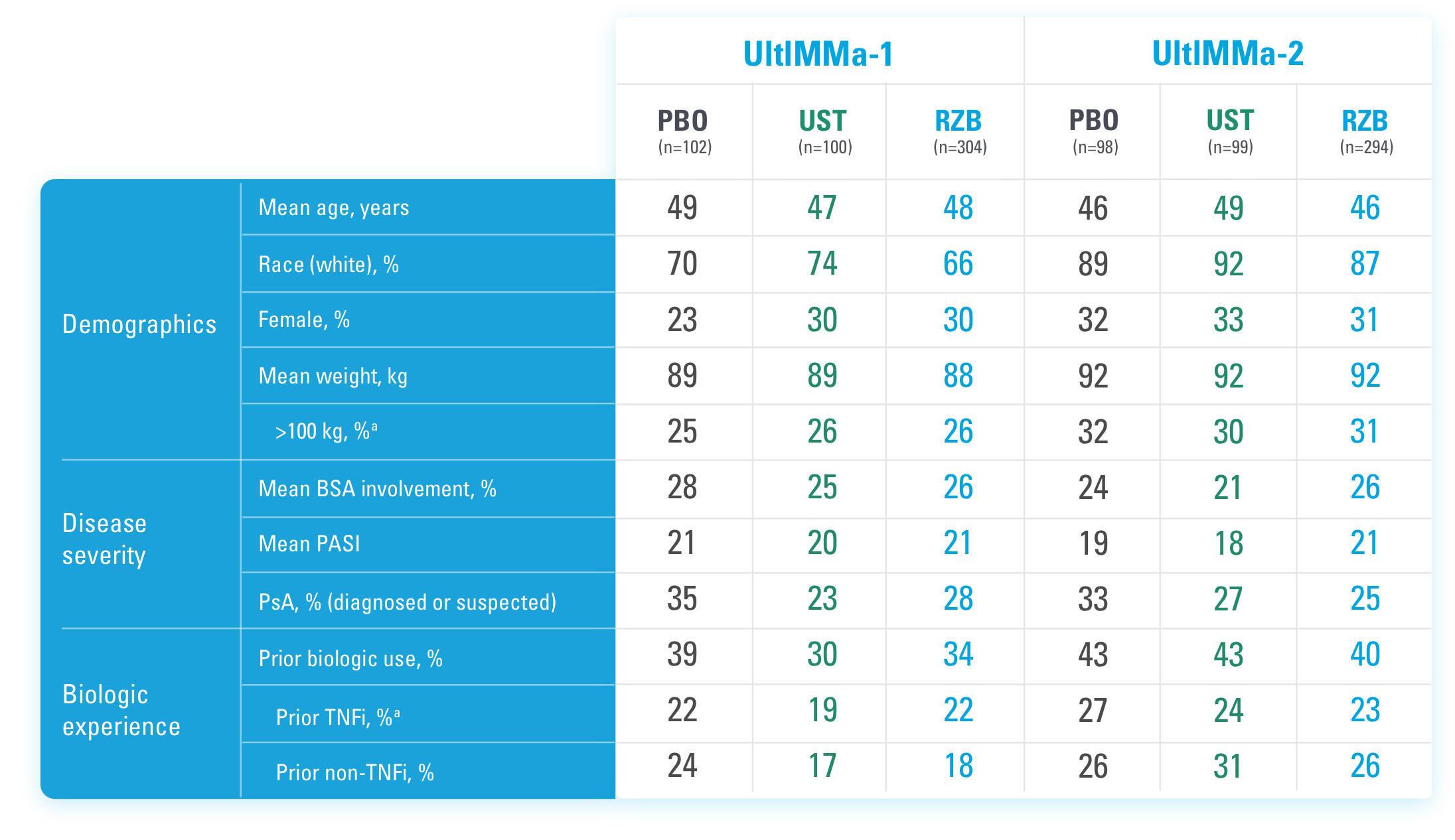
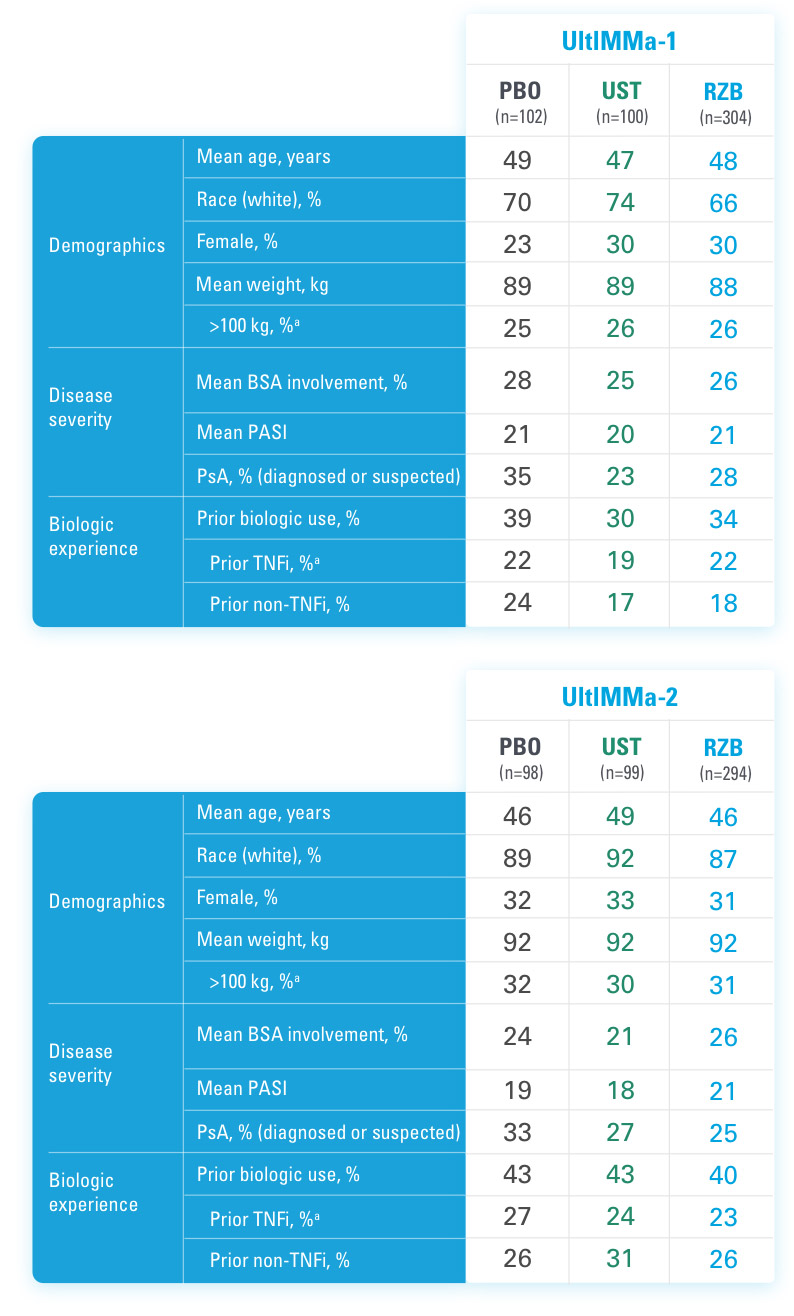
BSA=Body Surface Area
PASI=Psoriasis Area and Severity Index
PBO=Placebo
PsA=Psoriatic Arthritis
RZB=risankizumab-rzaa
TNFi=Tumor Necrosis Factor Inhibitor
UST=ustekinumab
aStratification factors at randomization.
Reference
US-SKZD-220459