


MULTIPLE DOMAINS IN ONE VIEW
GET THE FULL PICTURE BELOW
US-MULT-250253
The IL-23 inhibitor from AbbVie indicated for the treatment of adults with
active psoriatic arthritis (PsA) and for moderate to severe plaque psoriasis (Ps)
in adults who are candidates for systemic therapy or phototherapy.1
The IL-23 inhibitor from AbbVie indicated for the treatment of adults with: active psoriatic arthritis (PsA);
moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy; moderately
to severely active Crohn's disease (CD); or moderately to severely active ulcerative colitis (UC)
KEEPsAKE 1:
SKYRIZI 57% (n=483), PLACEBO 34% (n=481)
KEEPsAKE 2:
SKYRIZI 51% (n=224), PLACEBO 27% (n=219)
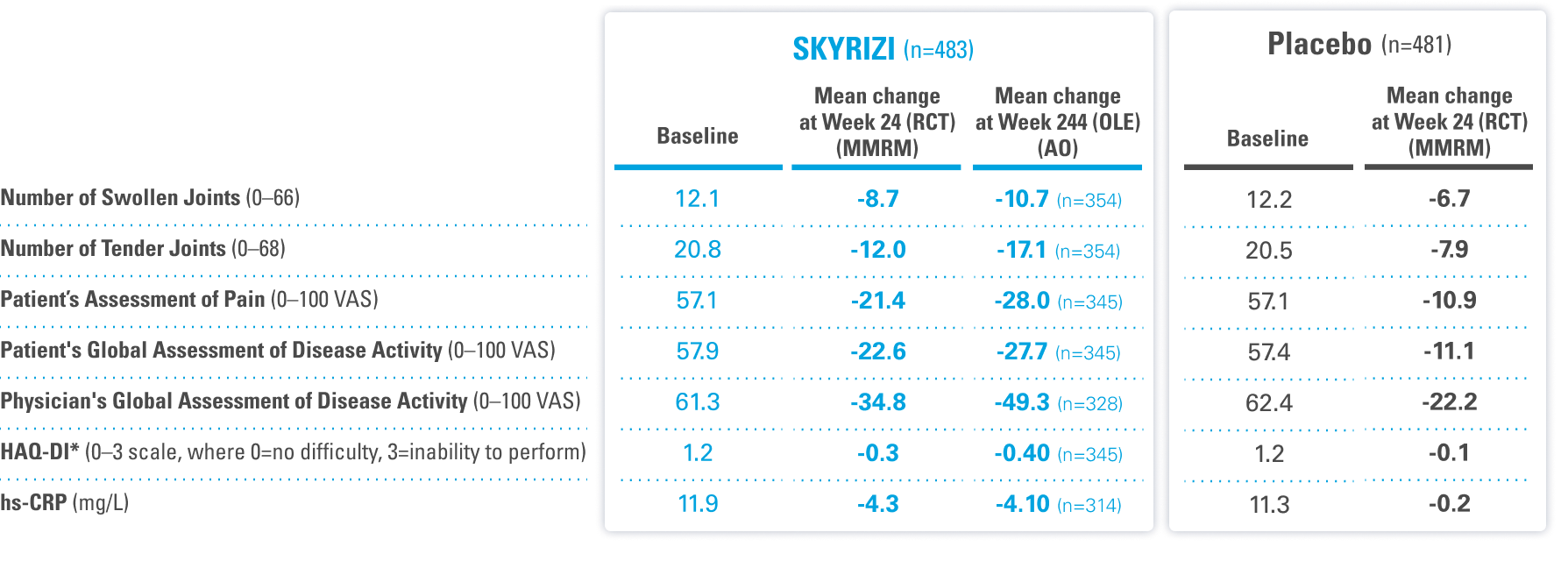
KEEPsAKE 1 (N=964) and KEEPsAKE 2 (N=443) were 2 randomized, double-blind, placebo-controlled studies that evaluated the efficacy and safety of SKYRIZI 150 mg vs placebo over 24 weeks with a long-term, open-label extension for up to an additional 292 weeks. Both studies enrolled adult patients with active psoriatic arthritis. In KEEPsAKE 1, the study population had an inadequate response or intolerance to at least 1 csDMARD, while in KEEPsAKE 2 patients had an inadequate response or intolerance to at least 1 biologic therapy OR to at least 1 csDMARD.1-3
GET THE FULL PICTURE BELOW
KEEPsAKE 1: csDMARD-IR
DATA LIMITATIONS: Data labeled as a ranked secondary endpoint were multiplicity-controlled for comparisons. All other comparisons were not adjusted for multiplicity; statistical significance has not been established.
OLE LIMITATIONS: An OLE may enrich long-term data, as patients intolerant or unresponsive to the drug drop out.
AS OBSERVED (AO) ANALYSIS: Patients with missing data at a specific time are not included, which may enrich the population and increase the response rates.
*Week 24 ranked secondary endpoint.5
ACR=American College of Rheumatology; AO=as observed; HAQ-DI=Health Assessment Questionnaire Disability Index; hs-CRP=high sensitivity C-reactive protein; MMRM=mixed-effect model for repeated measures; OLE=open-label extension; RCT=randomized controlled trial; VAS=visual analog scale
Enthesitis Resolution (LEI=0) (NRI-C)†a
Ranked key secondary endpoint: Pooled KEEPsAKE 1 and 2 data
48% with SKYRIZI (n=444) & 35% with placebo (n=448)
Dactylitis Resolution (LDI=0) (NRI-C)†a
Ranked key secondary endpoint: Pooled KEEPsAKE 1 and 2 data
68% with SKYRIZI (n=188) & 51% with placebo (n=204)
SJC ≥50% Improvement (NRI-C)§c
Post hoc analysis of ACR composite endpoint: KEEPsAKE 1
75% with SKYRIZI (n=483) & 59% with placebo (n=481)
TJC ≥50% Improvement (NRI-C)§c
Post hoc analysis of ACR composite endpoint: KEEPsAKE 1
65% with SKYRIZI (n=483) & 44% with placebo (n=481)
RADIOGRAPHIC RESULTS IN PsA
MEAN CHANGE IN mTSS (ANCOVA)‡b
Ranked key secondary endpoint: KEEPsAKE 1
Results were not statistically significant
0.23 with SKYRIZI (n=458) & 0.32 with placebo (n=457)
mTSS ≤0 (ANCOVA)‡b
Additional nonranked endpoint: KEEPsAKE 1
92% with SKYRIZI (n=458) & 88% with placebo (n=457)
RADIOGRAPHIC LIMITATION: KEEPsAKE 1 results did not establish a treatment effect on radiographic inhibition. The proportion of patients with no radiographic progression (mTSS ≤0.0) at Week 24 was a prespecified, nonranked endpoint; thus, no statistical or clinical conclusions can be drawn.
NAIL PSORIASIS IMPROVEMENT IN PsA
PGA-F: Mean Change from Baseline (MMRM)†d
Ranked key secondary endpoint: KEEPsAKE 1
-0.8 with SKYRIZI (n=280) & -0.4 with placebo (n=297)
At baseline, 64% of patients with PsA on SKYRIZI (n=309/483) and 71% on placebo (n=338/481) had presence of nail psoriasis.
PGA-F 0/1: PGA-F Score of 'Clear' or 'Minimal' (0/1) (AO)§‖d
Additional nonranked endpoint: KEEPsAKE 1
40% with SKYRIZI (n=182) & 19% with placebo (n=182)
SKYRIZI is not approved for mild plaque psoriasis.
§DATA LIMITATIONS: Proportion of patients with ≥50% tender joint count and swollen joint count improvement were post hoc analyses not prespecified or adjusted for multiplicity. PGA-F score 'clear' or 'minimal' was a prespecified nonranked endpoint not adjusted for multiplicity. No statistical or clinical conclusions can be made.
AO ANALYSIS: Patients with missing data at a specific time are not included, which may enrich the population and increase the response rates.
Radiographic Scoring Scale: The maximum possible scores are 320 for erosions, 208 for joint space narrowing, and 528 for the total score.
†P<0.001.
‡Radiographic endpoints were analyzed using an analysis of covariance model incorporating linear extrapolation to impute missing data.
‖PGA-F 0/1 with a ≥2-grade improvement. Among PsA patients with a PGA-F score of ≥2.0 (mild, moderate, or severe) at baseline.
aIntegrated results from KEEPsAKE 1 and KEEPsAKE 2 in patients with baseline presence of enthesitis (LEI>0) or dactylitis (LDI>0).
bAt baseline, the mean mTSS score was 13.0 in patients with PsA on SKYRIZI (n=483) and 13.5 in patients on placebo (n=481).
cTJC/SJC 50% improvement is defined as ≥50% reduction in TJC/SJC.
dAmong PsA patients with nail psoriasis, the mean baseline PGA-F score was 2.1 for SKYRIZI patients and 2.0 on placebo.
ACR=American College of Rheumatology; ANCOVA=analysis of covariance; AO=as observed; LDI=Leeds Dactylitis Index; LEI=Leeds Enthesitis Index; mTSS=modified total Sharp score; MMRM=mixed-effect model for repeated measures; NRI-C=nonresponder imputation incorporating multiple imputation to handle missing data due to COVID-19; PGA-F=Physician's Global Assessment of Fingernail Psoriasis; PsA=psoriatic arthritis; SJC=swollen joint count; TJC=tender joint count
KEEPsAKE 1: csDMARD-IR | ALL DATA ARE AS OBSERVED (AO) | OLE

TENDER JOINT COUNT¶
Post hoc analysis of ACR composite endpoint
93%
(n=354)
OF PATIENTS SAW
TJC improved by ≥50%#
AT WEEK 244

DACTYLITIS
97%
(n=141)
HAD
NO DACTYLITIS**
AT WEEK 244 (LDI=0)

ENTHESITIS
83%
(n=297)
HAD
NO ENTHESITIS**
AT WEEK 244 (LEI=0)

SWOLLEN JOINT COUNT¶
Post hoc analysis of ACR composite endpoint
97%
(n=354)
OF PATIENTS SAW
SJC improved by ≥50%#
AT WEEK 244

NAIL PSORIASIS¶
82%
(n=147)
OF PATIENTS
OBSERVED ’CLEAR’ or ‘MINIMAL’ PGA-F SCORE
AT WEEK 244 (PGA-F 0/1 with A ≥2 grade improvement)
Among PsA patients with PGA-F score ≥2.0 (mild, moderate, or severe) at baseline.

RADIOGRAPHIC RESULTS
Results were not statistically significant in mean change in mTSS at Week 24
88%
(n=337)
HAD
NO RADIOGRAPHIC PROGRESSION
AT WEEK 244 (CHANGE FROM BASELINE IN mTSS ≤0)
RADIOGRAPHIC LIMITATION: KEEPsAKE 1 results did not establish a treatment effect on radiographic inhibition. The proportion of patients with no radiographic progression (mTSS ≤0.0) at Week 24 was a prespecified, nonranked endpoint; thus, no statistical or clinical conclusions can be drawn.
¶DATA LIMITATIONS: Proportion of patients with ≥50% tender joint count and swollen joint count improvement were post hoc analyses not prespecified or adjusted for multiplicity. PGA-F score 'clear' or 'minimal' was a prespecified nonranked endpoint not adjusted for multiplicity. No statistical or clinical conclusions can be made.
OLE LIMITATIONS: An OLE may enrich long-term data, as patients intolerant or unresponsive to the drug drop out.
AO ANALYSIS: Patients with missing data at a specific time are not included, which may enrich the population and increase the response rates.
SKYRIZI is not approved for mild plaque psoriasis.
#TJC/SJC 50% improvement is defined as ≥50% reduction in TJC/SJC.
**Integrated results from KEEPsAKE 1 and KEEPsAKE 2 in patients with baseline presence of enthesitis (LEI>0) or dactylitis (LDI>0).
ACR=American College of Rheumatology; AO=as observed; csDMARD=conventional synthetic disease-modifying antirheumatic drug; IR=intolerance or inadequate response; LDI=Leeds Dactylitis Index; LEI=Leeds Enthesitis Index; mTSS=modified total Sharp score; NRI-C=nonresponder imputation incorporating multiple imputation to handle missing data due to COVID-19; OLE=open-label extension; PGA-F=Physician's Global Assessment of Fingernail Psoriasis; PsA=psoriatic arthritis; RCT=randomized controlled trial; SJC=swollen joint count; TJC=tender joint count
INDICATIONS AND IMPORTANT SAFETY INFORMATION FOR SKYRIZI® (risankizumab-rzaa)1 Indications Plaque Psoriasis: SKYRIZI is indicated for the treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy or phototherapy. Psoriatic Arthritis: SKYRIZI is indicated for the treatment of active psoriatic arthritis in adults. Crohn's Disease: SKYRIZI is indicated for the treatment of moderately to severely active Crohn's disease in adults. Ulcerative Colitis: SKYRIZI is indicated for the treatment of moderately to severely active ulcerative colitis in adults. |
Important Safety Information
Hypersensitivity Reactions
SKYRIZI® (risankizumab-rzaa) is contraindicated in patients with a history of serious hypersensitivity reaction to risankizumab-rzaa or any of the excipients. Serious hypersensitivity reactions, including anaphylaxis, have been reported with the use of SKYRIZI. If a serious hypersensitivity reaction occurs, discontinue SKYRIZI and initiate appropriate therapy immediately.
Infection
SKYRIZI may increase the risk of infection. Do not initiate treatment with SKYRIZI in patients with a clinically important active infection until it resolves or is adequately treated.
In patients with a chronic infection or a history of recurrent infection, consider the risks and benefits prior to prescribing SKYRIZI. Instruct patients to seek medical advice if signs or symptoms of clinically important infection occur. If a patient develops such an infection or is not responding to standard therapy, closely monitor and discontinue SKYRIZI until the infection resolves.
Tuberculosis (TB)
Prior to initiating treatment with SKYRIZI, evaluate for TB infection and consider treatment in patients with latent or active TB for whom an adequate course of treatment cannot be confirmed. Monitor patients for signs and symptoms of active TB during and after SKYRIZI treatment. Do not administer SKYRIZI to patients with active TB.
Hepatotoxicity in Treatment of Inflammatory Bowel Disease
Drug-induced liver injury was reported in a patient with Crohn’s disease who was hospitalized for a rash during induction dosing of SKYRIZI. For the treatment of Crohn's disease and ulcerative colitis, evaluate liver enzymes and bilirubin at baseline and during induction (12 weeks); monitor thereafter according to routine patient management. Consider an alternate treatment for patients with evidence of liver cirrhosis. Interrupt treatment if drug-induced liver injury is suspected, until this diagnosis is excluded. Instruct your patient to seek immediate medical attention if they experience symptoms suggestive of hepatic dysfunction.
Administration of Vaccines
Avoid use of live vaccines in patients treated with SKYRIZI. Medications that interact with the immune system may increase the risk of infection following administration of live vaccines. Prior to initiating SKYRIZI, complete all age-appropriate vaccinations according to current immunization guidelines.
Adverse Reactions
Most common (≥1%) adverse reactions associated with SKYRIZI in plaque psoriasis and psoriatic arthritis include upper respiratory infections, headache, fatigue, injection site reactions, and tinea infections.
In psoriatic arthritis phase 3 trials, the incidence of hepatic events was higher with SKYRIZI compared to placebo.
Most common (>3%) adverse reactions associated with SKYRIZI in Crohn’s disease are upper respiratory infections, headache, and arthralgia in induction and arthralgia, abdominal pain, injection site reactions, anemia, pyrexia, back pain, arthropathy, and urinary tract infection in maintenance.
Most common (≥3%) adverse reactions associated with SKYRIZI in ulcerative colitis are arthralgia in induction, and arthralgia, pyrexia, injection site reactions, and rash in maintenance.
Lipid Elevations: Increases from baseline and increases relative to placebo were observed at Week 4 and remained stable to Week 12 in patients treated with SKYRIZI in Crohn’s disease. Lipid elevations observed in patients with ulcerative colitis were similar to those in Crohn's disease.
Dosage Forms and Strengths: SKYRIZI (risankizumab-rzaa) is available in a 150 mg/mL prefilled syringe and pen, a 600 mg/10 mL single-dose vial for intravenous infusion, and a 180 mg/1.2 mL or 360 mg/2.4 mL single-dose prefilled cartridge with on-body injector.
INDICATIONS
Plaque Psoriasis: SKYRIZI is indicated for the treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy or phototherapy.
Psoriatic Arthritis: SKYRIZI is indicated for the treatment of active psoriatic arthritis in adults.
Crohn's Disease: SKYRIZI is indicated for the treatment of moderately to severely active Crohn's disease in adults.
Ulcerative Colitis: SKYRIZI is indicated for the treatment of moderately to severely active ulcerative colitis in adults.
Please see Full Prescribing Information.
US-SKZG-240258
REFERENCES
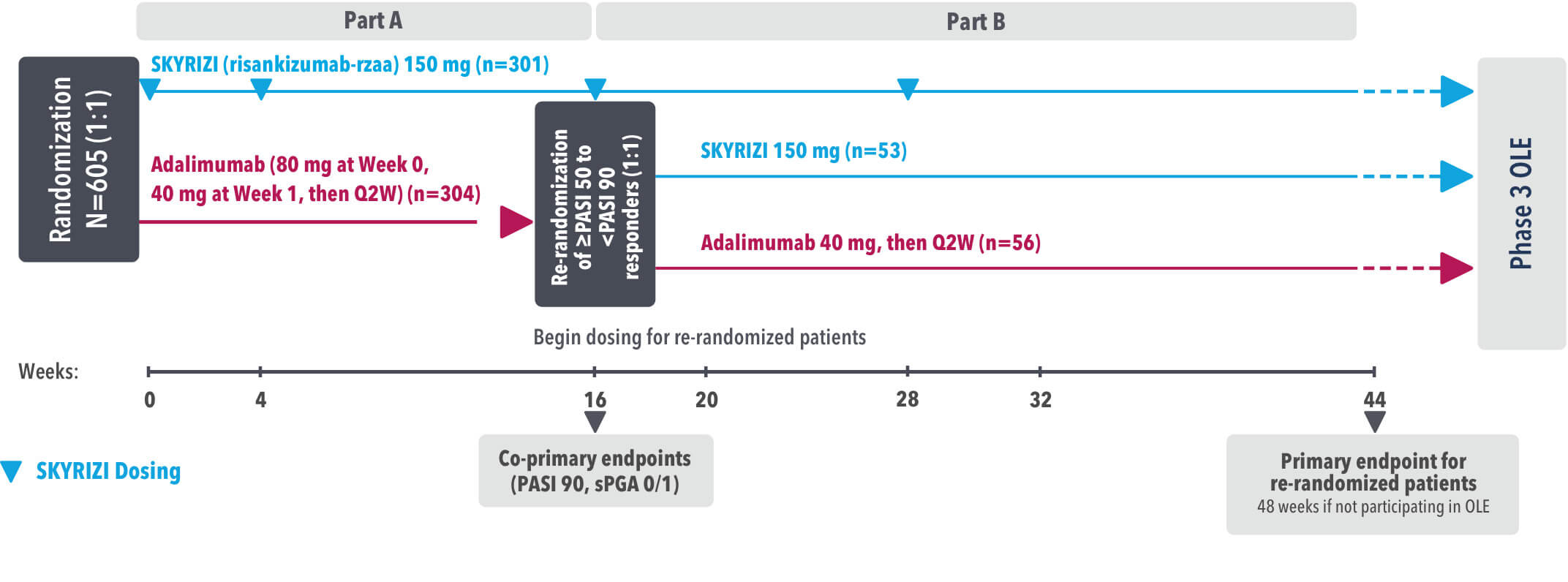
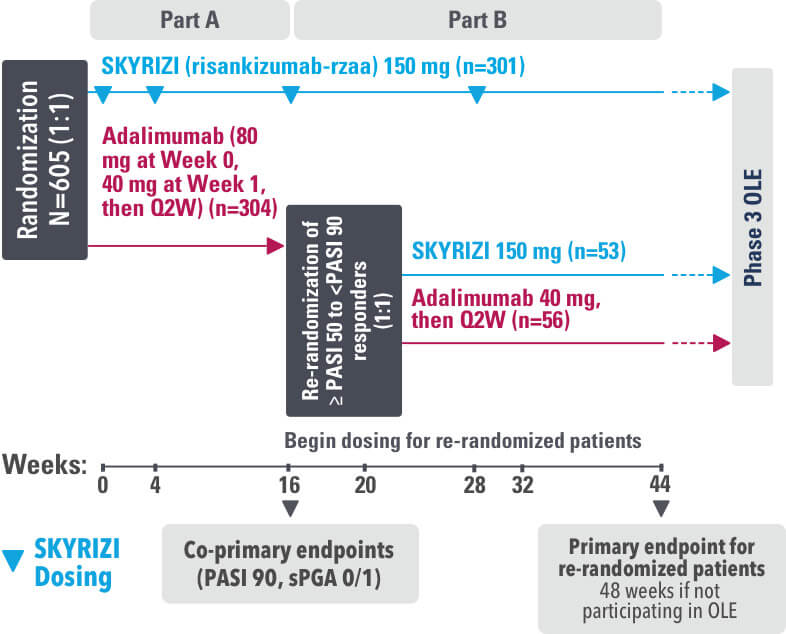
IMMvent was a Phase 3, randomized, double-blind, double-dummy, active-controlled study to evaluate the efficacy and safety of SKYRIZI (150 mg) compared to HUMIRA® (adalimumab) in adult patients with moderate to severe plaque psoriasis over 44 weeks.
Patients treated with adalimumab during Part A:
Part A
In the first phase, patients were randomized 1:1 to either SKYRIZI (150 mg), given as a subcutaneous injection at Weeks 0 and 4 and every 12 weeks thereafter or HUMIRA, given as a subcutaneous injection, with an initial dose of 80 mg followed by 40 mg every other week starting 1 week after the initial dose over 44 weeks.
The Part A co-primary endpoints were
Part B
Patients originally randomized to SKYRIZI received it throughout the study (Parts A & B). Among patients originally randomized to receive HUMIRA, those with a PASI 50 but less than PASI 90 response were re-randomized 1:1 to switch to SKYRIZI or continue HUMIRA.
The Part B primary endpoint was
Key secondary endpoints included
Key inclusion criteria
OLE=open-label extension
PASI=Psoriasis Area Severity Index
PASI 90=≥90% improvement in Psoriasis Area Severity Index
PASI 100=100% improvement in Psoriasis Area Severity Index
Q2W=once every 2 weeks
sPGA=static Physician's Global Assessment
Click to see HUMIRA® (adalimumab) Indication and Important Safety Information, including BOXED WARNING for Serious Infections and Malignancy
OLE=Open-Label Extension
PASI=Psoriasis Area and Severity Index
PASI 90=≥90% improvement in Psoriasis Area and Severity Index
PASI 100=100% improvement in Psoriasis Area and Severity Index
Q2W=Once every 2 weeks
sPGA=static Physician's Global Assessment
REFERENCE

ADA=adalimumab
BSA=body surface area
PASI=Psoriasis Area Severity Index
PsA=psoriatic arthritis
RZB=risankizumab-rzaa
TNFi=tumor necrosis factor inhibitor
REFERENCES
US-SKZR-260027
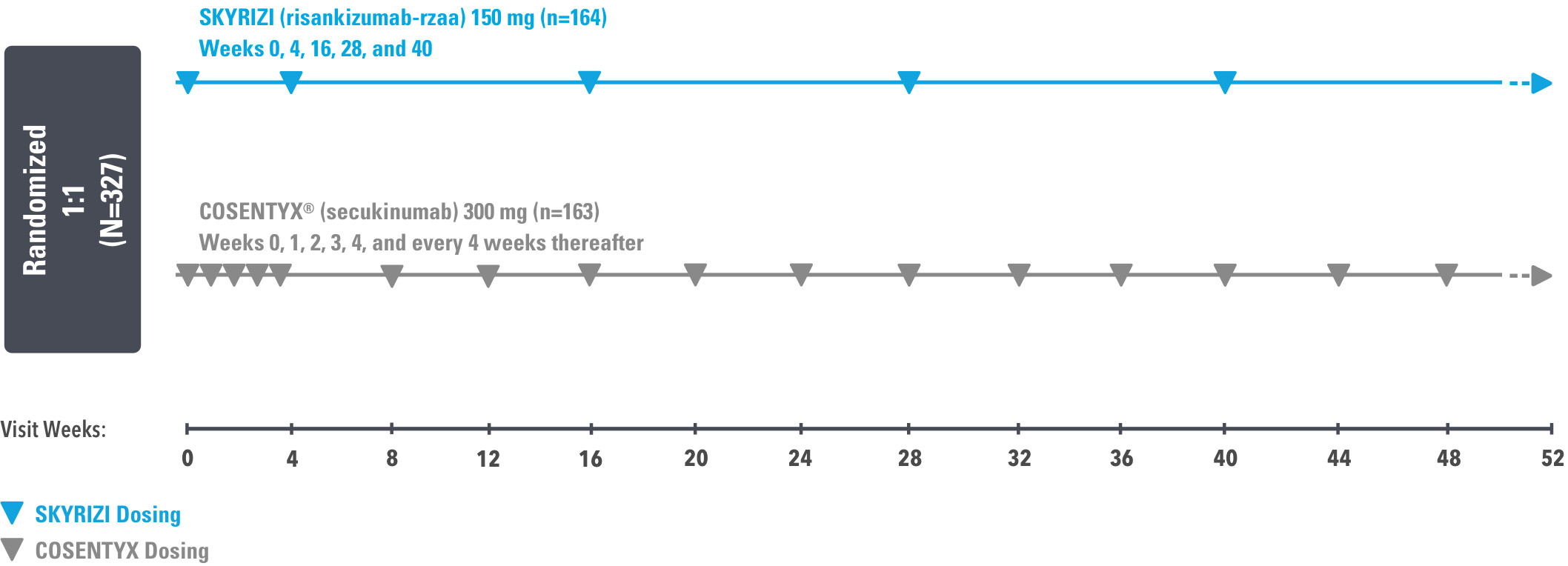
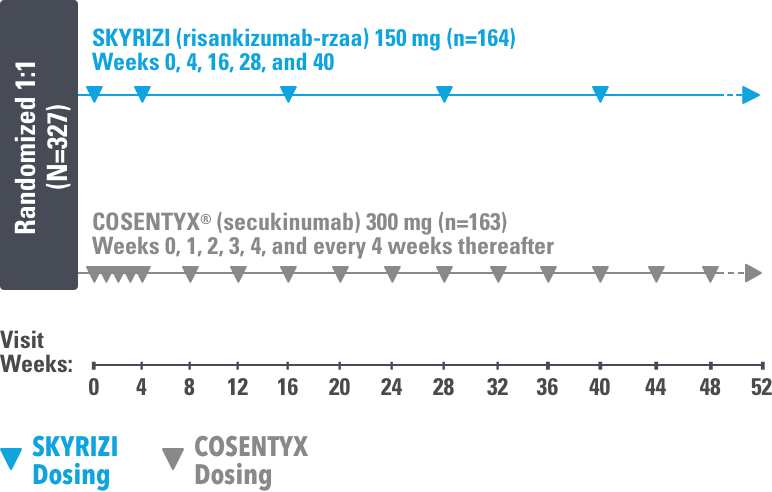
IMMerge was a Phase 3, global, multicenter, randomized, open-label, efficacy–assessor-blinded, active-comparator study that evaluated the safety and efficacy of SKYRIZI 150 mg vs COSENTYX 300 mg in moderate to severe plaque psoriasis subjects, who were candidates for systemic therapy.
The primary endpoints were
Ranked secondary endpoints (all superiority)
Key inclusion criteria
Sourcing
In this study, 46 patients outside of the US received non–US-licensed secukinumab.
Data regarding comparability between US and non-US secukinumab are not publicly available.
BSA=body surface area
PASI=Psoriasis Area Severity Index
sPGA=static Physician's Global Assessment
REFERENCE

BSA=body surface area
PASI=Psoriasis Area Severity Index
RZB=risankizumab-rzaa
SEC=secukinumab
sPGA=static Physician's Global Assessment
aMean baseline body weight was 92 kg in the secukinumab group and 91.1 kg in the risankizumab group.2
bStratification factors at randomization.
REFERENCES
US-SKZR-260027
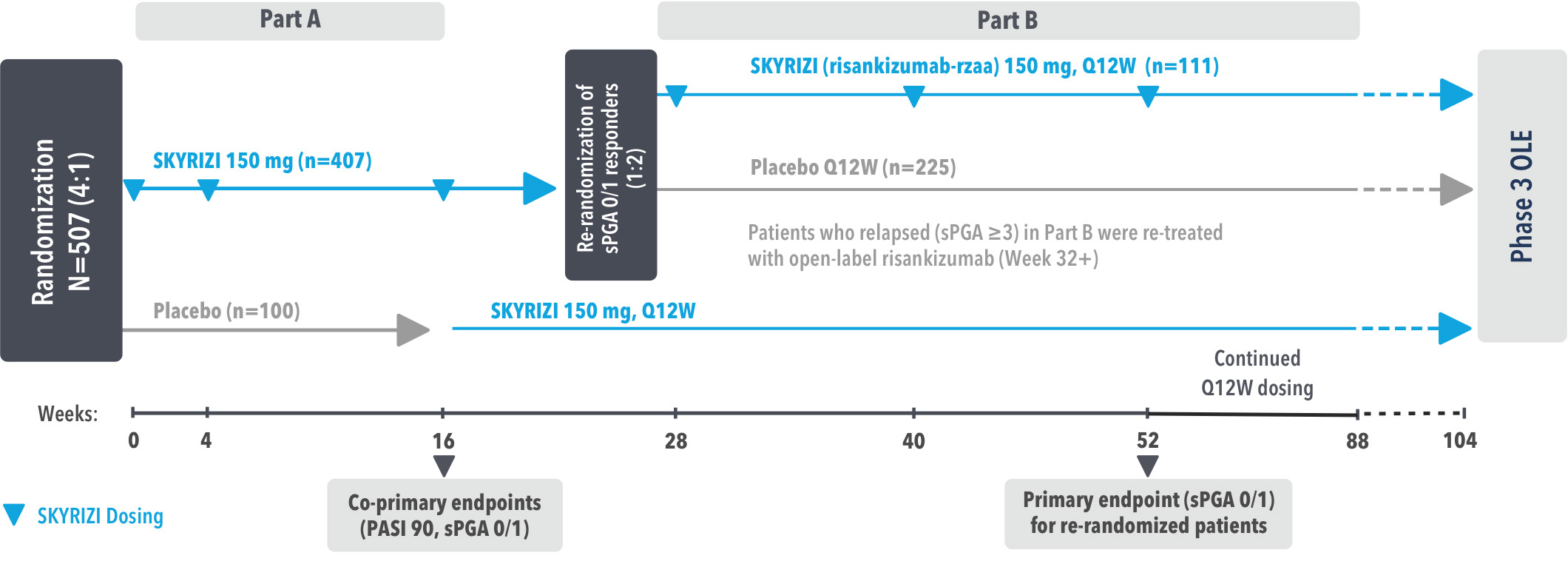
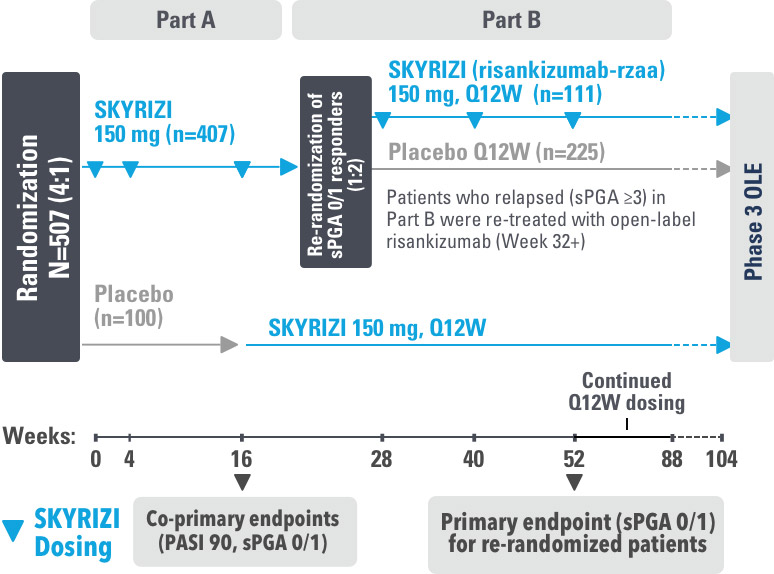
IMMhance was a Phase 3, multicenter, randomized, double-blind, placebo-controlled study to evaluate the impact of treatment withdrawal and re-treatment of SKYRIZI compared to placebo in adult patients with moderate to severe plaque psoriasis.
Part A
In the first phase, patients were randomized 4:1 to SKYRIZI (150 mg), given as a subcutaneous injection at baseline, 4 weeks later, and every 12 weeks thereafter, or placebo.
The Part A co-primary endpoints were
Part B
In the second phase of this study (Week 28 through Week 104), patients originally randomized to SKYRIZI who achieved sPGA 0/1 at Week 28 were re-randomized (1:2) to SKYRIZI (maintenance) or placebo (withdrawal). Beginning at Week 32, patients with sPGA ≥2 continued on SKYRIZI (150 mg) once every 12 weeks up to Week 88, with a final follow-up at Week 104.
The Part B primary endpoint was
Key inclusion criteria
Key secondary endpoints included
DLQI=Dermatology Life Quality Index
OLE=Open-Label Extension
PASI=Psoriasis Area and Severity Index
PASI 75=≥75% improvement in Psoriasis Area and Severity Index
PASI 90=≥90% improvement in Psoriasis Area and Severity Index
PASI 100=100% improvement in Psoriasis Area and Severity Index
Q12W=Once every 12 weeks
sPGA=static Physician's Global Assessment
REFERENCES
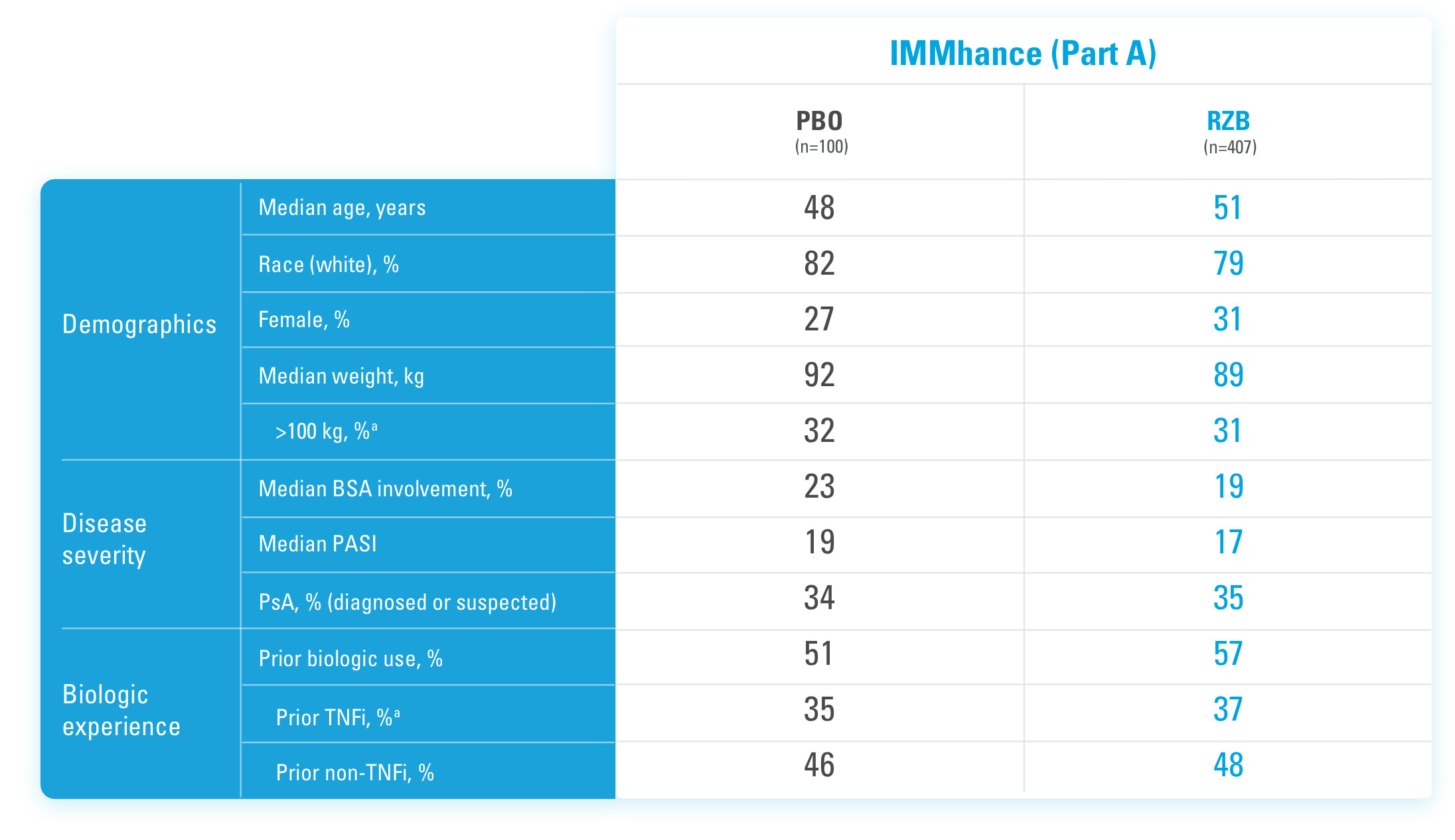
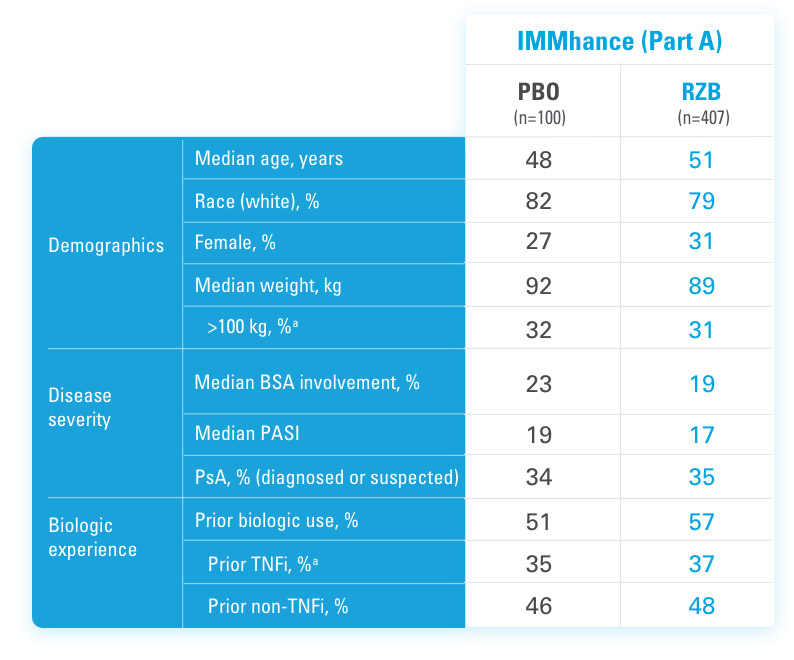
BSA=Body Surface Area
PASI=Psoriasis Area and Severity Index
PBO=Placebo
PsA=Psoriatic Arthritis
RZB=Risankizumab-rzaa
TNFi=Tumor Necrosis Factor Inhibitor
aStratification factors at randomization.
REFERENCES
US-SKZR-260027
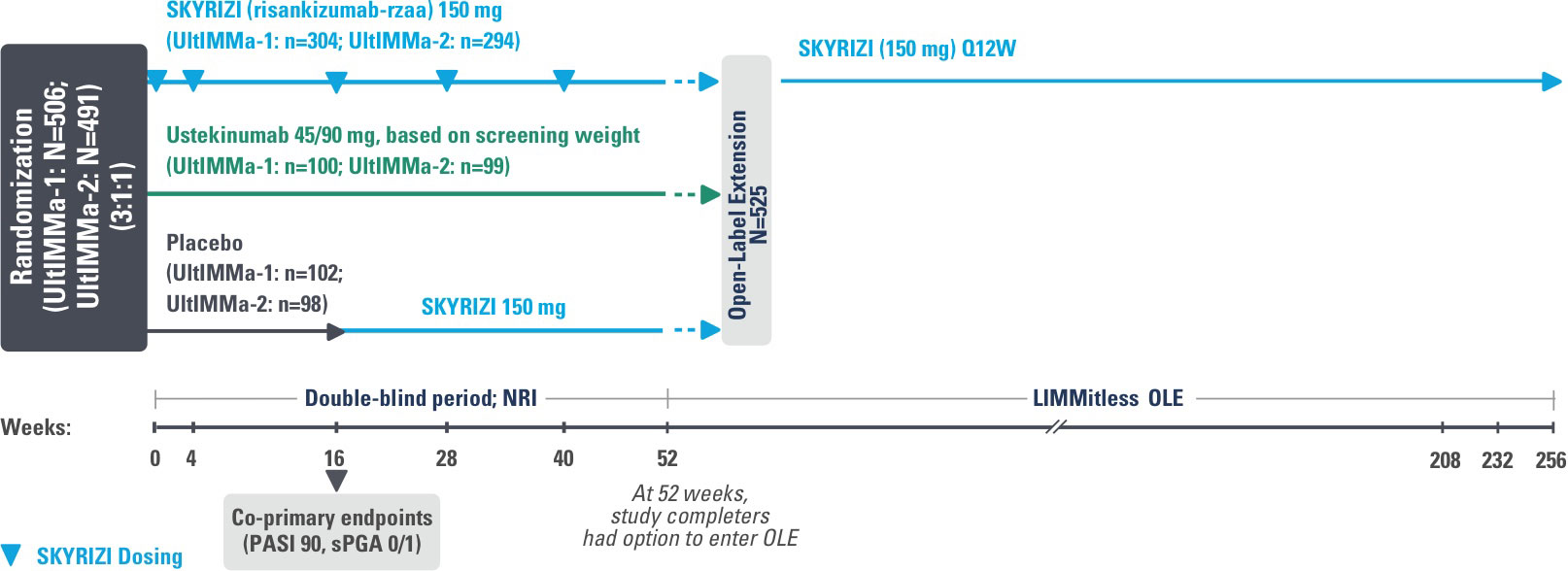
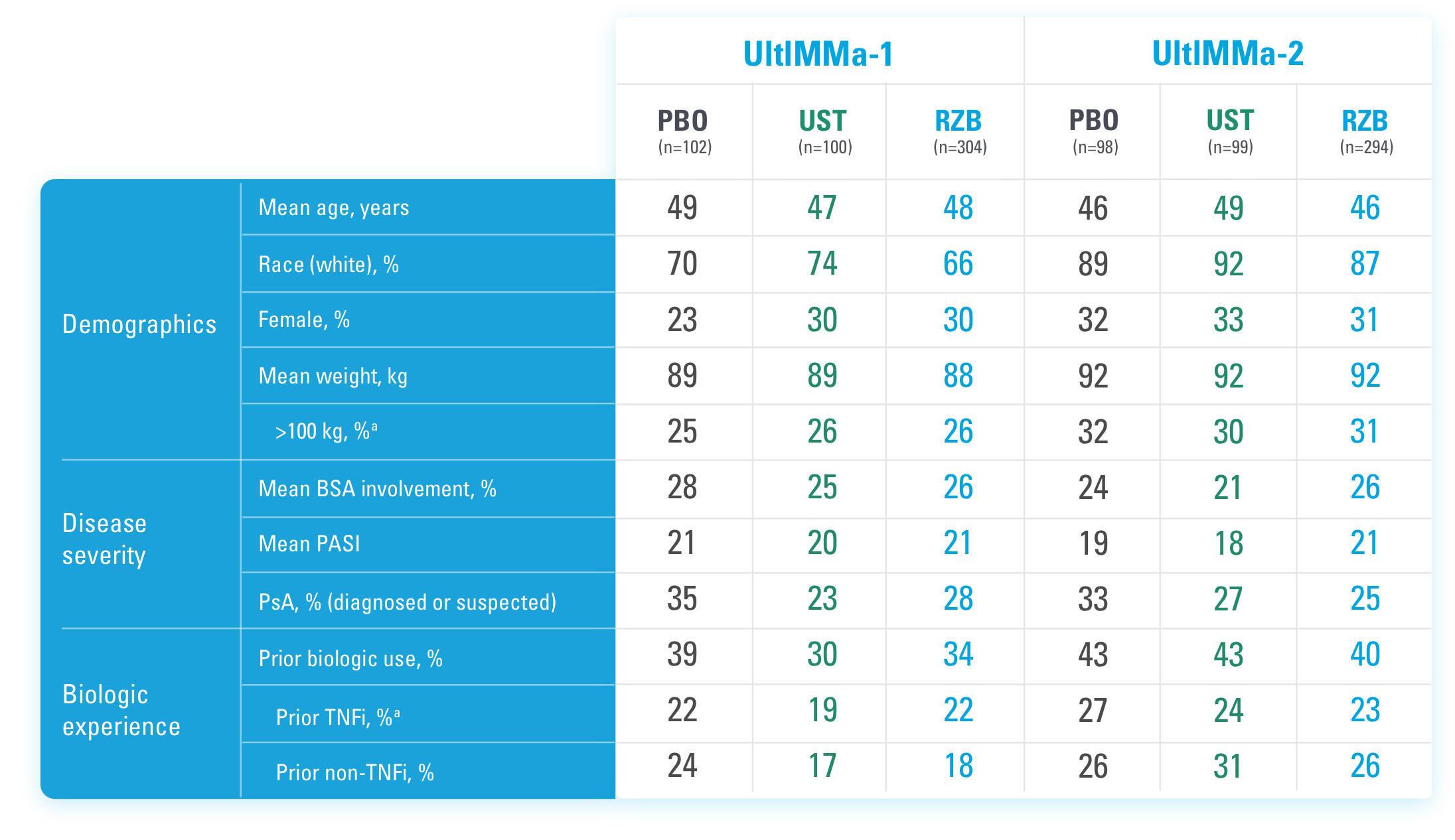
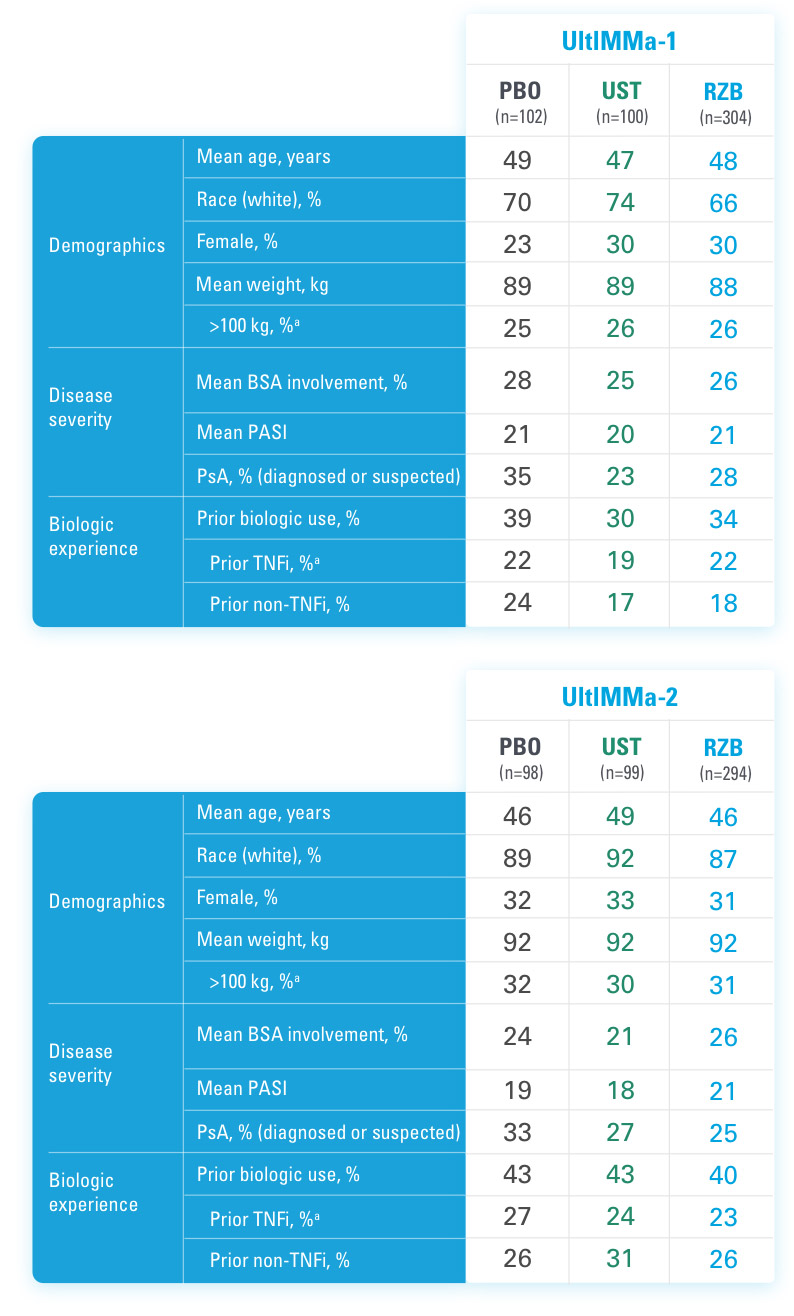
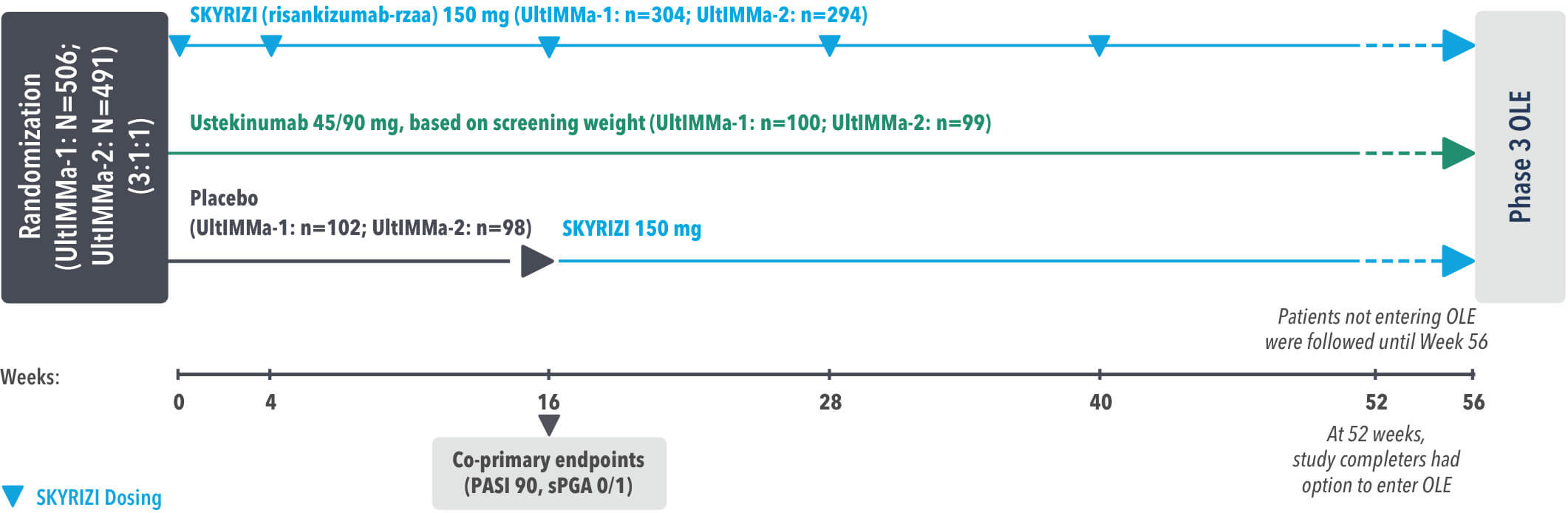
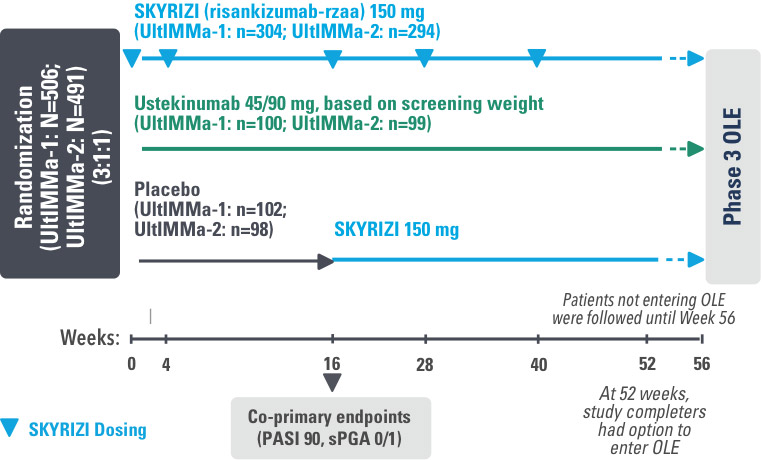
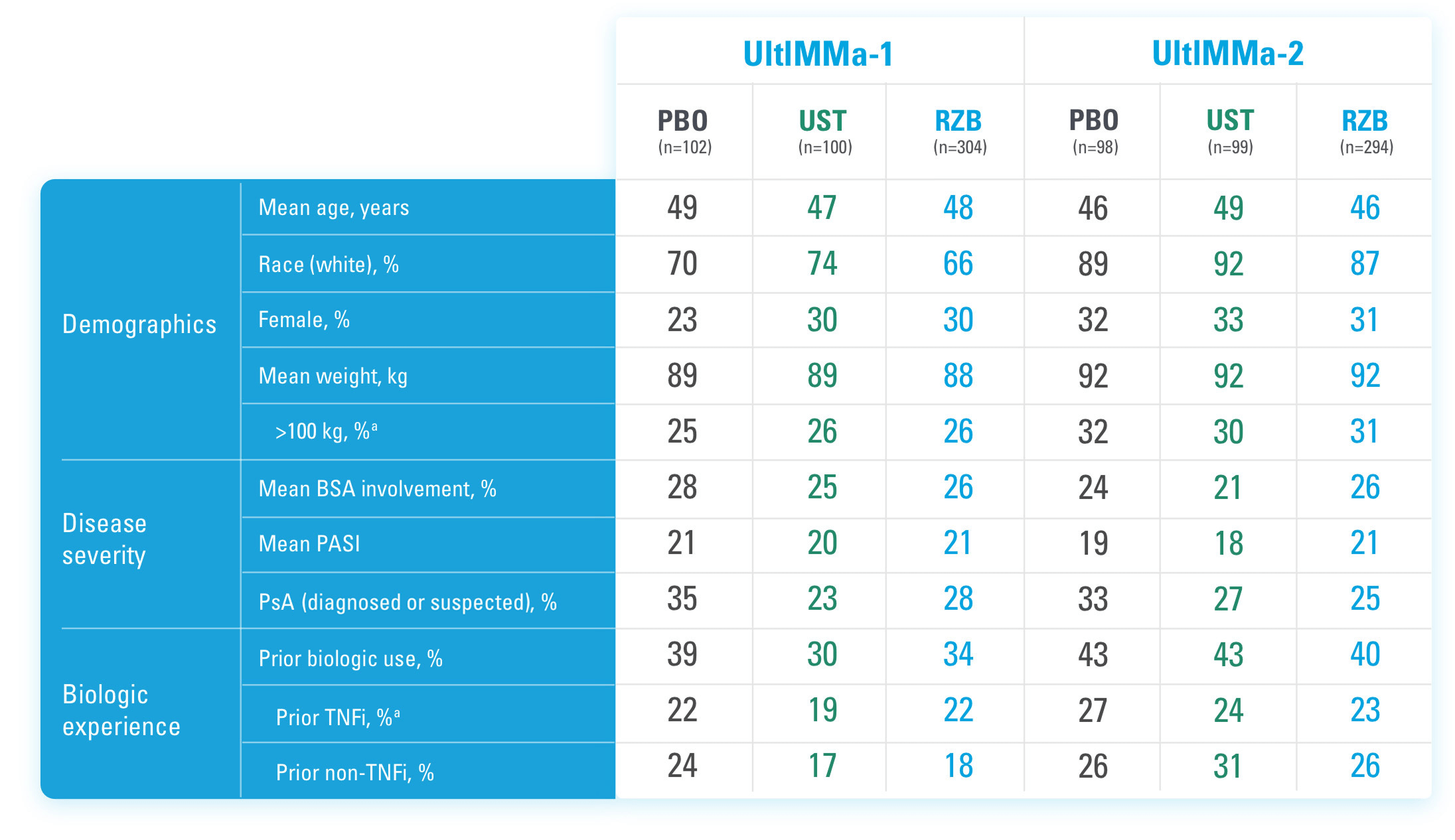
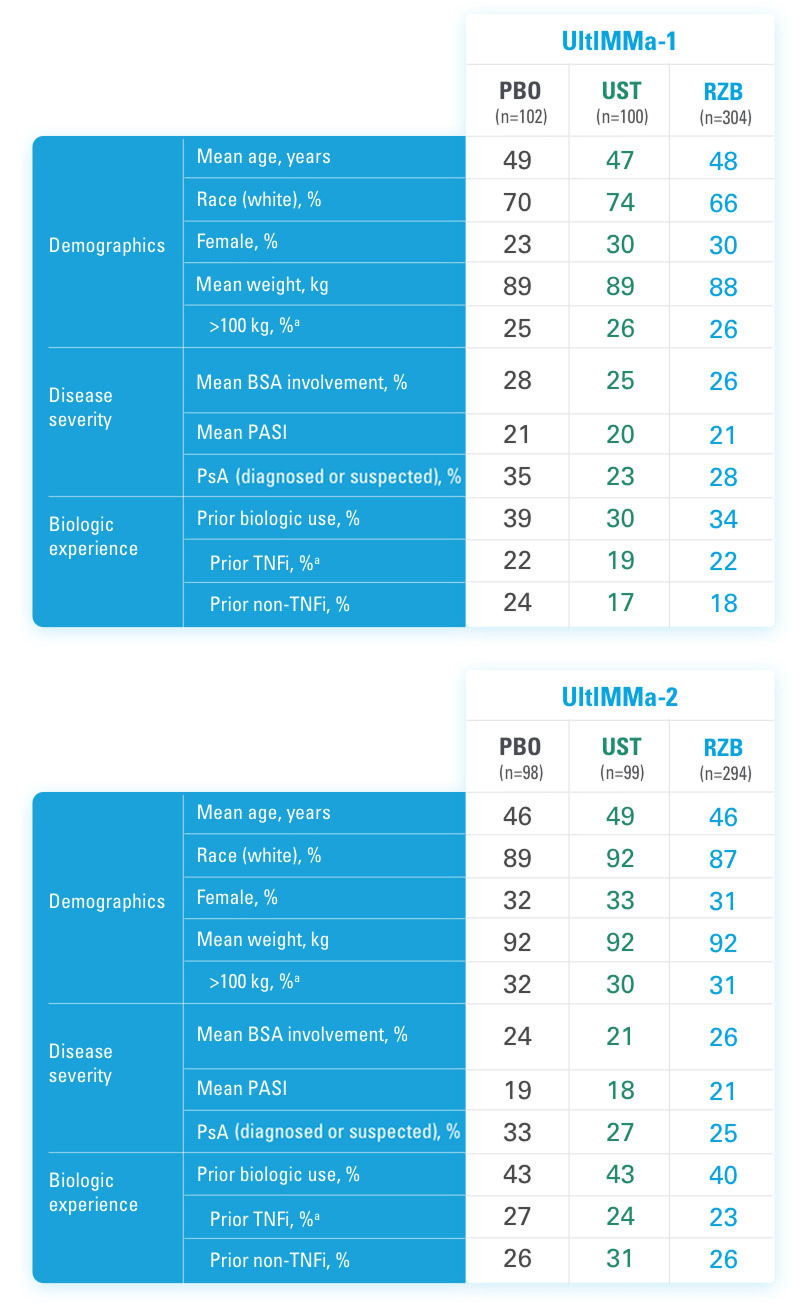
UltIMMa-1 (N=506) and UltIMMa-2 (N=491) were replicate Phase 3, randomized, double-blind, placebo- and active-controlled studies to evaluate the efficacy and safety of SKYRIZI (150 mg) vs placebo over 16 weeks and biologic active control (45 mg or 90 mg, based on screening weight) over 52 weeks in adult patients with moderate to severe plaque psoriasis. SKYRIZI (150 mg) was given as 2 subcutaneous injections at Weeks 0, 4, 16, 28, and 40. Patients were randomized 3:1:1 to receive SKYRIZI, ustekinumab, or placebo. At Week 16, patients on placebo were switched to SKYRIZI.
LIMMitless is an ongoing, single-arm, multicenter, open-label extension study evaluating the long-term efficacy and safety of SKYRIZI (150 mg). Patients who completed UltIMMa-1 or -2, IMMvent, or IMMhance were eligible to participate.
Active comparator
The active comparator (ustekinumab) used for these studies was sourced from the European Union.
OLE=Open-Label Extension
PASI=Psoriasis Area and Severity Index
PASI 90=≥90% improvement in Psoriasis Area and Severity Index
PASI 100=100% improvement in Psoriasis Area and Severity Index
sPGA=static Physician's Global Assessment
The co-primary endpoints were
Key secondary endpoints included
Key inclusion criteria
OLE=Open-Label Extension
PASI=Psoriasis Area and Severity Index
PASI 90=≥90% improvement in Psoriasis Area and Severity Index
PASI 100=100% improvement in Psoriasis Area and Severity Index
sPGA=static Physician's Global Assessment
REFERENCES
BSA=Body Surface Area
PASI=Psoriasis Area and Severity Index
PBO=Placebo
PsA=Psoriatic Arthritis
RZB=Risankizumab-rzaa
TNFi=Tumor Necrosis Factor Inhibitor
UST=Ustekinumab
aStratification factors at randomization.
REFERENCE
US-SKZR-260027
UltIMMa-1 (N=506) and UltIMMa-2 (N=491) were replicate Phase 3, randomized, double-blind, placebo- and active-controlled studies to evaluate the efficacy and safety of SKYRIZI (150 mg) vs placebo over 16 weeks and biologic active control (45 mg or 90 mg, based on screening weight) over 52 weeks in adult patients with moderate to severe plaque psoriasis. SKYRIZI (150 mg) was given as 2 subcutaneous injections at Weeks 0, 4, 16, 28, and 40. Patients were randomized 3:1:1 to receive SKYRIZI, ustekinumab, or placebo. At Week 16, patients on placebo were switched to SKYRIZI.
Active comparator
The active comparator (ustekinumab) used for these studies was sourced from the European Union.
The co-primary endpoints were
Key secondary endpoints included
Key inclusion criteria
OLE=open-label extension
PASI=Psoriasis Area Severity Index
PASI 90=≥90% improvement in Psoriasis Area Severity Index
PASI 100=100% improvement in Psoriasis Area Severity Index
sPGA=static Physician's Global Assessment
REFERENCES
BSA=body surface area
PASI=Psoriasis Area Severity Index
PBO=placebo
PsA=psoriatic arthritis
RZB=risankizumab-rzaa
TNFi=tumor necrosis factor inhibitor
UST=ustekinumab
aStratification factors at randomization.
REFERENCE:
US-SKZR-260027
UltIMMa-1 (N=506) and UltIMMa-2 (N=491) were replicate Phase 3, randomized, double-blind, placebo- and active-controlled studies to evaluate the efficacy and safety of SKYRIZI (150 mg) vs placebo over 16 weeks and biologic active control (45 mg or 90 mg, based on screening weight) over 52 weeks in adult patients with moderate to severe plaque psoriasis. SKYRIZI (150 mg) was given as 2 subcutaneous injections at Weeks 0, 4, 16, 28, and 40. Patients were randomized 3:1:1 to receive SKYRIZI, ustekinumab, or placebo. At Week 16, patients on placebo were switched to SKYRIZI.
Active comparator
The active comparator (ustekinumab) used for these studies was sourced from the European Union.
The co-primary endpoints were
Key secondary endpoints included
Key inclusion criteria
OLE=open-label extension
PASI=Psoriasis Area Severity Index
PASI 90=≥90% improvement in Psoriasis Area Severity Index
PASI 100=100% improvement in Psoriasis Area Severity Index
sPGA=static Physician's Global Assessment
REFERENCES
BSA=body surface area
PASI=Psoriasis Area Severity Index
PBO=placebo
PsA=psoriatic arthritis
RZB=risankizumab-rzaa
TNFi=tumor necrosis factor inhibitor
UST=ustekinumab
aStratification factors at randomization.
REFERENCE:
US-SKZR-260027

KEEPsAKE 1: csDMARD-IR. KEEPsAKE 2: Mixed population (50% csDMARD-IR, 50% Bio-IR)
KEEPsAKE 1 (N=964) and KEEPsAKE 2 (N=443) were 2 randomized, double-blind, placebo-controlled studies to evaluate the efficacy and safety of SKYRIZI (150 mg) vs placebo over 24 weeks with an open-label extension for up to an additional 204 weeks in adult patients with active psoriatic arthritis.
In both studies, patients were randomized to receive SKYRIZI 150 mg or placebo at Weeks 0, 4, and 16. Starting from Week 28, all patients received SKYRIZI every 12 weeks. 59.6% of patients from both studies were receiving concomitant MTX, 11.6% were receiving concomitant non-biologic DMARDs other than MTX, and 28.9% were receiving SKYRIZI monotherapy.
Patients in KEEPsAKE 1 previously experienced an inadequate response, intolerance, or contraindication to ≥1 csDMARD. Patients in KEEPsAKE 2 were bio-IR and/or csDMARD-IR.
In both studies, similar responses were seen regardless of concomitant non-biologic DMARD use, number of prior non-biologic DMARDs, age, gender, race, and BMI. In KEEPsAKE 2, responses were seen regardless of prior biologic therapy.
*The first n-value is for KEEPsAKE 1; the second n-value is for KEEPsAKE 2.
†At Week 16, patients classified as nonresponders (defined as not achieving at least a 20% improvement in either or both tender joint count and swollen joint count at both Week 12 and Week 16 compared to baseline) had the option to add or modify rescue concomitant medications/therapy. Starting at Week 36, patients classified as nonresponders were discontinued from study drug.
‡To maintain the blind to the original treatment at Week 24, patients randomized to placebo received blinded risankizumab 150 mg, and patients randomized to risankizumab received blinded placebo.
Primary endpoint
Select ranked secondary endpoints
Non-ranked secondary endpoints
Key inclusion criteria
ACR=American College of Rheumatology
Bio-IR=inadequate response or intolerance to a biologic
BMI=body mass index
csDMARD=conventional synthetic disease-modifying antirheumatic drugs
csDMARD-IR=intolerance or inadequate response to conventional synthetic disease-modifying antirheumatic drug(s)
LDI=Leeds Dactylitis Index
LEI=Leeds Enthesitis Index
mTSS=modified total Sharp Score
MTX=methotrexate
NRI-C=non-responder imputation incorporating multiple imputation to handle missing data due to COVID-19
OLE=open-label extension
PASI=Psoriasis Area Severity Index
PBO=placebo
RZB=risankizumab-rzaa
aAmong patients with ≥3% body surface area affected by psoriasis at baseline.
bNot included in KEEPsAKE 2.
cAmong patients with nail psoriasis at baseline.
dDefined as LEI=0 among patients with LEI >0 at baseline. Prespecified analysis of pooled data from the KEEPsAKE 1 and KEEPsAKE 2 trials (RZB, n=444; PBO, n=448).
eDefined as LDI=0 among patients with LDI >0 at baseline. Prespecified analysis of pooled data from the KEEPsAKE 1 and KEEPsAKE 2 trials (RZB, n=188; PBO, n=204).
REFERENCES

aBased on 68 joints.
bBased on 66 joints.
BMI=body mass index
BSA=body surface area
csDMARD=conventional synthetic disease-modifying antirheumatic drugs
mTSS=modified Total Sharp Score
MTX=methotrexate
NSAID=nonsteroidal anti-inflammatory drug
PBO=placebo
PsA=psoriatic arthritis
RZB=risankizumab-rzaa
BMI=body mass index
BSA=body surface area
csDMARD=conventional synthetic disease-modifying antirheumatic drugs
mTSS=modified Total Sharp Score
MTX=methotrexate
NSAID=nonsteroidal anti-inflammatory drug
PBO=placebo
PsA=psoriatic arthritis
RZB=risankizumab-rzaa
REFERENCES
US-SKZR-260027
US-SKZR-260027
To achieve an ACR20, 50, or 70 response, a patient must have at least a 20%, 50%, or 70%, respectively, improvement in tender and swollen joint counts and three of five scores of individual elements:

REFERENCES
1. SKYRIZI [package insert]. North Chicago, IL: AbbVie Inc. 2. Mease PJ, Antoni CE, Gladman DD, Taylor WJ. Psoriatic arthritis assessment tools in clinical trials. Ann Rheum Dis. 2005;64(suppl II):ii49-ii54. 3. Data on file, AbbVie Inc. ABVRRTI71868. 4. Mease P, Strand V, Gladman D. Functional impairment measurement in psoriatic arthritis: importance and challenges. Semin Arthritis Rheum. 2018;48(3):436-448.
US-SKZR-260027
ACROSS 4 PIVOTAL TRIALS

Click to see HUMIRA® (adalimumab) Indication and Important Safety Information, including
BOXED WARNING for Serious Infections and Malignancy. See Full Prescribing Information.
ACTIVE COMPARATOR
The ustekinumab used as a biologic active control in UltIMMa-1 and UltIMMa-2 was sourced from the European Union. Comparability between non–US-approved ustekinumab and US-approved ustekinumab has not been established. See Full Prescribing Information for US-approved ustekinumab, which reflects different rates of adverse events from those observed for EU-approved ustekinumab in the UltIMMa trials.
Safety analyses were performed using a safety analysis set (all patients who received ≥1 dose of study drug). No safety data for adalimumab or placebo were obtained beyond Week 16.
aIncludes data from UltIMMa-1, UltIMMa-2, IMMhance, and IMMvent studies.
bIncludes data from UltIMMa-1, UltIMMa-2, and Phase 2 study 1311.2.
cSKYRIZI (150 mg), adalimumab, and placebo were only evaluated in Phase 3 trials; the ustekinumab group includes Phase 3 patients (N=199) in addition to Phase 2 patients (n=40).
dIncludes data from IMMvent study.
eIncludes data from UltIMMa-1, UltIMMa-2, and IMMhance studies.
IBD=inflammatory bowel disease; MACE=major adverse cardiovascular event; NMSC=nonmelanoma skin cancer; Ps=psoriasis; TB=tuberculosis.
STELARA is a registered trademark of Johnson & Johnston. See US prescribing information for further information.
REFERENCES
US-SKZR-260027

Active Comparator
The ustekinumab used as a biologic active control in UltIMMa-1 and UltIMMa-2 was sourced from the European Union. Comparability between non–US-approved ustekinumab and US-approved ustekinumab has not been established. See Full Prescribing Information for US-approved ustekinumab, which reflects different rates of adverse events from those observed for EU-approved ustekinumab in the UltIMMa trials.
Safety analyses were performed using a safety analysis set (all patients who received ≥1 dose of study drug). No safety data for adalimumab or placebo were obtained beyond Week 16.
aIncludes data from UltIMMa-1 and UltIMMa-2 studies.
STELARA is a registered trademark of Johnson & Johnson. See US Prescribing Information for further information.
REFERENCES
US-SKZR-260027

*The first n-value is for KEEPsAKE 1; the second n-value is for KEEPsAKE 2.
†At Week 16, subjects classified as nonresponders (defined as not achieving at least a 20% improvement in either or both tender joint count and swollen joint count at both Week 12 and Week 16 compared to baseline) had the option to add or modify rescue concomitant medications/therapy. Starting at Week 36, subjects classified as nonresponders were discontinued from study drug.
‡To maintain the blind to the original treatment at Week 24, subjects randomized to placebo received blinded SKYRIZI 150 mg, and subjects randomized to SKYRIZI received blinded placebo.
KEEPsAKE 1: csDMARD-IR. KEEPsAKE 2: Mixed population (~50% csDMARD-IR, ~50% Bio-IR)
csDMARD-IR population: Inadequate response (lack of efficacy after minimum 12-week duration of therapy) or intolerance to previous or current treatment with at least 1 csDMARD at maximally tolerated dose; Bio-IR population: Inadequate response (lack of efficacy after minimum 12-week duration of therapy) or intolerance to treatment with 1 or 2 biologic therapies intended to treat PsA
KEEPsAKE 1 (N=964) and KEEPsAKE 2 (N=443) were 2 randomized, double-blind, placebo-controlled studies that evaluated the efficacy and safety of SKYRIZI (150 mg) vs placebo over 24 weeks with an open-label extension for up to an additional 292 weeks in adult patients with active psoriatic arthritis.
In both studies, subjects were randomized to receive SKYRIZI 150 mg or placebo at Weeks 0, 4, and 16. Starting at Week 28, all subjects received SKYRIZI every 12 weeks. 59.6% of subjects from both studies received concomitant MTX, 11.6% received concomitant nonbiologic DMARDs other than MTX, and 28.9% received SKYRIZI monotherapy.
In both studies, similar responses were seen regardless of concomitant nonbiologic DMARD use, number of prior nonbiologic DMARDs, age, gender, race, and BMI.
In KEEPsAKE 2, responses were seen regardless of prior biologic therapy.
In KEEPsAKE 1, bilateral radiographs of hands and feet were included at screening, baseline, Week 24, Week 52, Week 100, Week 148, Week 196, and Week 244.
Primary endpoint
Ranked key secondary endpoints
Nonranked secondary endpoints
Key inclusion criteria
aIn the subset of subjects with a body surface area (BSA) ≥3% at baseline.
bIn the subset of subjects with nail psoriasis at baseline.
cIn the subset of subjects with enthesitis at the LEI sites at baseline.
dIn the subset of subjects with dactylitis at the LDI sites at baseline.
ACR=American College of Rheumatology; ACR20/50/70=≥20%/50%/70% improvement in tender joint count, swollen joint count, and at least 3 other core criteria; Bio-lR=inadequate response or intolerance to a biologic; BMI=body mass index; csDMARD=conventional synthetic disease-modifying antirheumatic drug; csDMARD-IR=intolerance or inadequate response to conventional synthetic disease-modifying antirheumatic drug; DMARD=disease-modifying antirheumatic drug; HAQ-Dl=Health Assessment Questionnaire Disability Index; LDI=Leeds Dactylitis Index; LEI=Leeds Enthesitis Index; MDA=minimal disease activity; mNAPSl=modified Nail Psoriasis Severity Index; mTSS=modified total Sharp score; MTX=methotrexate; OLE=open-label extension; PASI 90=≥90% improvement in Psoriasis Area Severity Index; PsA=psoriatic arthritis
REFERENCES
US-SKZR-260027

aBased on 68 joints.
bBased on 66 joints.
BMI=body mass index; BSA=body surface area; csDMARD=conventional synthetic disease-modifying antirheumatic drug; DMARD=disease-modifying antirheumatic drug; HAQ-DI=Health Assessment Questionnaire Disability Index; LDI=Leeds Dactylitis Index; LEI=Leeds Enthesitis Index; mTSS=modified total Sharp score; MTX=methotrexate; NSAID=nonsteroidal anti-inflammatory drug; PASl=Psoriasis Area Severity Index; PsA=psoriatic arthritis
REFERENCES
US-SKZR-260027